Welcome to sympathetikey’s page.
Contributor score: 1600
Comments ...
thisisfine
Same - the bleeding thing pushed me over to psoriasis as well. Oops.
+6
temmy
the distribution of the other lesions, forearm, face, ear, scalp..is not characteristic for psoriasis.
+8
hyperfukus
the scalp and ear are actually very common for psoriasis IRL the key is more of the fact that its in areas with UV exposure...actually UV Therapy is found to be helpful in treating some pts w/Psoriasis. Lastly the appearance and lots of things bleed if they were trying to go for auspitz sign it would have tiny dots of bright red blood with slightly touching it
+7
hyperfukus
oh last thing psoriasis itches! they said no itching
+7
drzed
Those locations may be common IRL, but on step 1, if they want you to think psoriasis, the illness script is going to be someone in their 30s (autoimmune age) with symmetric cutaneous plaques that have a silvery scale on the extensor surfaces.
In this case, the age and non-classic description (location, type of lesion) made me steer away from psoriasis.
+3
amy
Why not squamous cell carcinoma itself?
+
amy
nevermind, I think the 8 year history explained it
+
sahusema
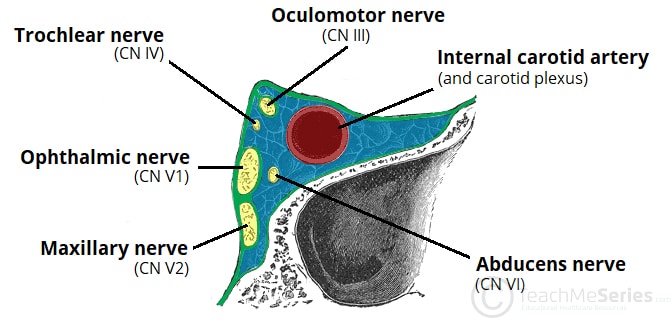
I know you're right. I was just so uncomfortable picking an answer with "inferior rectus" because damage to the inferior rectus does nothing to explain the clinical findings of impaired upward gaze. Unless the muscle is physically stuck and can't relax or something
+7
emmy2k21
Agreed. Why would a dysfunctional inferior rectus contribute to impaired upward gaze??? I eliminated that answer choice and got it wrong :(
+2
dr_jan_itor
in the last sentence it asks you to assume an "entrapment", so it is actually the inferior rectus which is the cause of the upward gaze palsy. The entrapped muscle is functionally trapped in it's shortened position, thereby not allowing the orbit to gaze upward.
+16
chandlerbas
bam! dr_jan_itor just cleaned up that confusion
+2
weirdmed51
Why inferior oblique then? Doesn’t IO helps to look up ?
+1
freemanpeng
May be IR is stronger than IO in downward gaze?
+
cbreland
"intermittent" made me think IBS as well
+
heenaasnani
Was i the only one to think that it could be carcinoid syndrome as it is episodic?
+
heenaasnani
I thought it is a carcinoid tumor and not a syndrome yet, as the patient has only GI manifestations. Can someone explain why can't it be that?
+
fatboyslim
@heenaasnani even if it was, there is no answer choice targeting treatment of carcinoid, which would be octreotide (somatostatin analog). I agree with you though, carcinoid was on my differential while reading the question.
+
cbreland
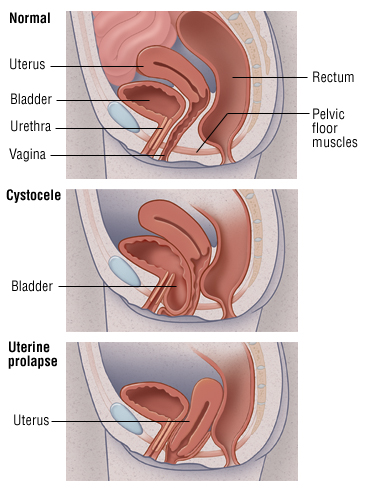
How would you rule out uterine prolapse?
+
mkayman
and just for completeness, rectocele would have a posterior vaginal wall bulge
+2
mkayman
and just for completeness, rectocele would have a posterior vaginal wall bulge
+
handsome
what is the meaning/significance
of 16.8difficult score?
+
yb_26
@at0xibolic, I think you won this competition on finding better picture lol thanks
+6
j44n
that was my exact reasoning
+3
zoggybiscuits
I thought it was spleen but the fact that hematocrit was 24% 4 HOURs later made me think otherwise. It was my understanding that the spleen would bleed you out quick!
+1
need_answers
couldn't also be ruptured spleen because they said intraperitoneal fluid and everything else is retroperitoneal ??
+4
peqmd
Spleen is most commonly ruptured in blunt trauma so along with myelofibrosis and being kicked on the left side it's just asking to be ruptured
+3
limberry
@need_answers the bladder is intraperitoneal, not retro
+
limberry
bladder is sub*peritoneal, sorry
+
jsanmiguel415
Also unilateral and periorbital;, can differentiate from migraines because of it's short duration (30 minutes to a few hours vs migraines which is hours to days). Relationship to seasonal/allergies as well
+
aaftabsethi1
How the hell did pediculus spread in the class . Who is having head to head contact there ?
+
impostersyndromel1000
they probably were assigned group projects where the teacher asked them to put their heads together ;-)
+1
lamhtu
To be even clearer, this sounds like **Fanconi syndrome, which has lead to Type II RTA**
+12
yb_26
To be even clearer: Wilson disease => Fanconi syndrome => type II (proximal) RTA
+
yng
I don't thin this is Wilson (copper in descemet layer of cornea). This is cystinosis (crystal in the cornea) --> Fanconi Syndrome --> Type II (PCT) RTA.
+
meningitis
Could you elaborate? Is this related to: less "preload" from mother circulation causes lowered HR?
+
meningitis
Or backflow of blood and causes a Reflex Bradycardia? still confused on this question.
+
kentuckyfan
So I think the subtle difference in choice E is that there would be a negative CHRONOTROPIC effect, no inotropic effect (contractility).
+10
maxillarythirdmolar
if anything, inotrophy could go UP not down as diastole prolongs and LVEDV increases --> Starling equation bullshit
+
motherfucker2
If it was a woman would be a dysgerminoma. Seminomas have excellent prognosis and highly radiosensitive. MCC testicular tumor
+6
drschmoctor
Spunky fun fact:
In a normal adult male >1,000 sperm are made per heartbeat.
+15
an1
@drschmoctor we're really heavily targeting the wrong gender for birth control then...
+3
someduck3
I'm not 100% about this so take it with a grain of salt. But i was confused about why there would be a systolic murmur. I think its b/c prolonged ASD would eventually cause pulmonic stenosis which would present as a systolic murmur. But besides that I super agree with @sympathetikey
+
paulkarr
Low key was hoping for someone to try and argue this one...
+
an1
I was stuck between Aortic insufficiency or ASD. I opted for ASD because Aortic insufficiency is usually referred to when there's aneurysm or something, leading to the valve being insufficient to close and causing regurgitation (which is a diastolic murmur). I've seen this word used mostly with regurgitation, just a thought
+
yb_26
even if it would be steroid in the list, if NSAIDs are contraindicated => we give Colchicine, and if pt can't tolerate Colchicine as well => then we use steroids
+6
usmlecharserssss
uptodate - try to avoid steroid therapy in gout , in this case patient has aspirin (NSAID) allergy , so second line is Colchicine , not Allopurinol, which is for chronic management. This case is not RARE and a lot of people sits on Colchicine therapy even if they do not have NSAID problems. Colchicine also First line treatment for Familial Mediterranean Fever, prevent exacerbations.
+4
littletreetrunk
I think this makes total sense, but how does it not ALSO stop fast axonal transport?
+5
laminin
axonal transport is transport of organelles bidirectionally along the axon in the cytoplasm since myelin is on the outside of the axon demyelination doesn't affect this process.
source: https://en.wikipedia.org/wiki/Axonal_transport
"Axonal transport, also called axoplasmic transport or axoplasmic flow, is a cellular process responsible for movement of mitochondria, lipids, synaptic vesicles, proteins, and other cell parts to and from a neuron's cell body, through the cytoplasm of its axon."
+5
yotsubato
axonal transport is mediated by kinesin and dynein. Microtubule toxins like vincristine block these
+4
drdoom
@littletreetrunk "axonal transport" is movement of bulk goods via microtubules (which run from soma to terminus); ions, on the other hand, move in an "electrical wave" that we call an action potential! no axonal (microtubular) transport required! in other words, de-myelination will have no effect on the transport of bulk goods; but it will really mess up how fast "electrical waves" traverse the neuron!
+
gabeb71
The give away is the Fever, Pancytopenia, and Hepatosplenomegaly after being bitten by an insect and developing the sore.
+16
tallerthanmymom
I got this question directly after the other visceral leishmania question and it made me second guess everything I thought I knew.
+11
qball
Don't forget they like to infect macrophages.
+1
ls3076
how can we actually be expected to know vaccination schedules... there must be some other reason the answer is correct
+5
cbreland
I don't think we need to know that the vaccination schedules, but that the only other answer with a vaccine was adenovirus. I figured that there would have more symptoms if she had adenovirus (plus didn't fit the typical military recruit/swimmer demographic)
+1
koko
Why does it have to be something with a vaccine?
RSV Is extremely common in babies,shouldn’t screen for that?
+1
makingstrides
I didn't get my hep B vaccine until I was a teen
+2
srmtn
it is related to the screening during pregnancy, nothing to do with vaccines.
+2
ergogenic22
there is a delayed onset hemolytic transfusion reaction which should be evaluated with direct cooms test.
https://www.ncbi.nlm.nih.gov/books/NBK448158/
+7
baja_blast
Dang, I didn't know that was the same thing as a direct Coombs test. I guess it makes sense in hindsight. Thanks!
+
sars
Theres a UWORLD question with a table displaying the different types of hemolytic reactions. Don't know the question ID. Agree with delayed hemolytic transfusion reaction due to formation of antibodies against donor non ABO antigens. Typically presents as an asymptomatic patient or mild symptoms (jaundice, anemia). Different from an acute hemolytic transfusion reaction, which is against ABO antigens.
+3
lukin4answer
Delayed Hemolytic transfusion reaction is Host IgG against donor's RBC Rh or minor blood group Ag.(details on UW 17780), we do direct COOMB test where we add "ANTI-immunoGLOBULIN Ab" to patient's blood, if RBC is coated with IgG, then they agglutinates. As we add "ANTI-immunoGLOBULIN", hence this direct coomb test is called = DIRECT ANTIGLOBULIN test (DAT).
I got it wrong too, then dug through.
UW Q 317, 891, 1851 mentions COOMB TEST= Direct ANTIGLOBULIN TEST :/ :/ :/
& it's usually the INDIRECT BILLIRUBIN that rises with hemolysis, not direct (option C)
+2
jcmed
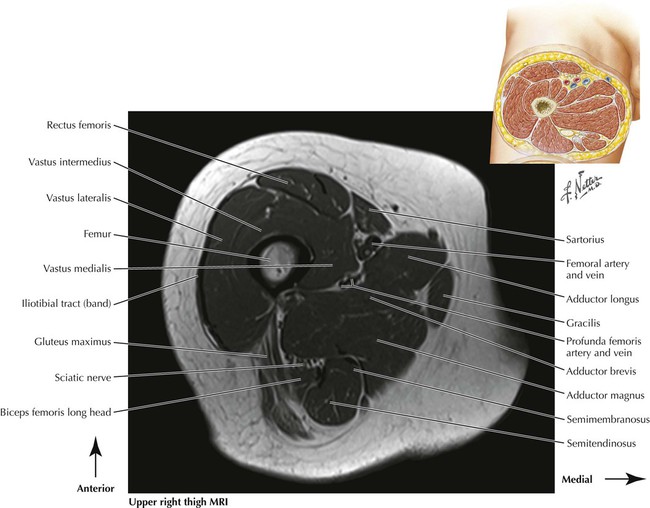
Was so close to picking vastus intermedius
+1
Subcomments ...
meningitis
The above explanation is correct (disregarding the hard to read and unprofessional dialect) but just in case anyone was wondering:
chromatin-negative= Just a quick way of knowing it was a boy. The term applies to the nuclei of cells in normal males as well as those in individuals with certain chromosomal abnormalities
+17
yotsubato
Turner syndrome patients are also chromatin negative as well though....
+6
sympathetikey
I didn't know a complication post-meningitis was lack of humor.
+6
sympathetikey
Ah, didn't read the last line. Yeah, that is taking it a bit far
+32
niboonsh
yall are haters. this is the first explanation that has ever made sense to me
+7
whoissaad
How does chormatin-negative indicate a normal cell? Isn't chormatin just condensed DNA?
+2
cienfuegos
According to this paper most individuals with Turner Syndrome are chromatin negative: "One of the initial laboratory procedures used to confirm or rule out this diagnosis involves a sex chromatin determination from a buccal smear. Cells from the lining of the mouth are stained for the presence or absence of X-chromatin or Barr bodies, which represent a portion of an inactivated X chromosome. The typical Turner’s syndrome patient, who has 45 chromosomes and only one sex chromosome (an X), has no Barr bodies and is, therefore, X-chromatin negative.
This abnormal X-chromatin negative finding in the majority of Turner’s syndrome females is similar to the result found in a normal male, who also has only one X chromosome, and differs from the X-chromatin positive condition observed in the normal female, who has two X chromosomes. Occasionally, the patient with features of Turner’s syndrome is found to be X-chromatin positive."
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6233891/
+2
hyperfukus
i really hate haters this is awesome!
+2
selectuw
to add to the above, free testosterone is aromatized to estrogen leading to breast development
+1
misrao
Is the free testosterone not creating male internal or external gentalia because of the defect in androgen receptors?
+1
niboonsh
Im mad at how simple this question actually is
+7
sahusema
Incidence is measured from those AT RISK. People with the disease are not considered to be at risk. So 2500 - 500 = 2000 people at-risk. Of those 2000, within one year 200 develop the disease. So 200/2000 of the at-risk population develop the disease. 20/2000 = 10% = incidence
+3
skonys
Must be Florida State University....
+
l0ud_minority
What if they got chlamydia again how would this change the numbers?
+
sympathetikey
Also, just thinking out loud, in the case of RCC, it's the kidney tissue that's dysplastic & moving, so technically the renal artery itself isn't dysplastic, right?
+
paperbackwriter
@usmleuser007 very good point regarding the venous vs arterial circulation that I neglected to consider!
+
yotsubato
How is that NOT posterior to middle concha? bad question
+11
sympathetikey
@yotsubato - That would have been if it was the spehnoid sinus (I got it wrong too btw)
+2
sahusema
Sphenoethmoidal RECESS not sphenoethmoidal SINUS
+4
neonem
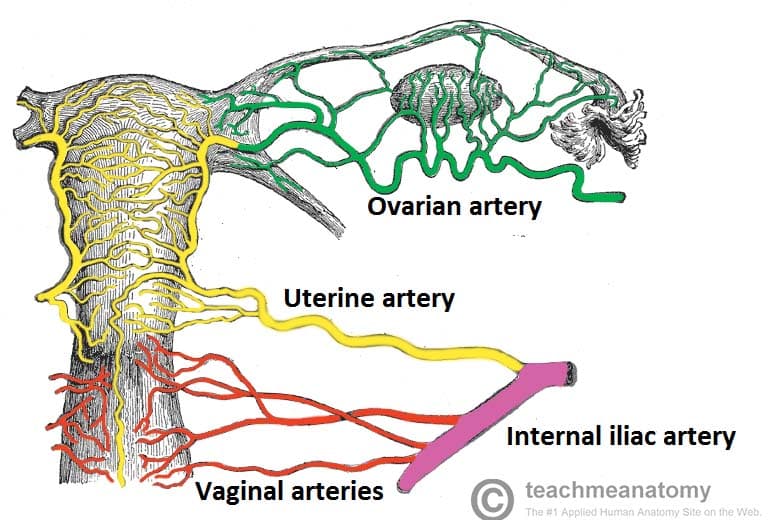
This sounds like a case of acute endometritis. In any case, uterus is supplied by uterine artery (branch of internal iliac artery) with collateral flow from ovarian artery (comes right off aorta). I don't think there are any branches of external iliac artery into the pelvis; it becomes femoral artery once it passes under inguinal ligament.
+4
tsl19
Here's a picture that I found helpful [Female Reproductive Tract arterial supply] (https://teachmeanatomy.info/wp-content/uploads/Blood-Supply-to-Female-Reproductive-Tract.jpg)
+18
hungrybox
tripped me up cause I didn't know the names :(
+17
angelaq11
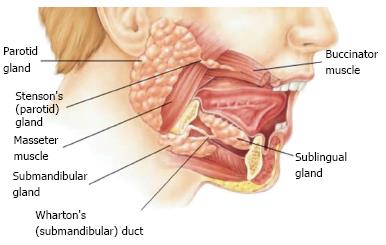
omg, same here! I thought, well, I don't know of any duct that connects the pancreas to the liver, so...2nd part of the duodenum it is :'( :'(
+8
alimd
actually Ampulla of Vater is located in the 2nd part of the duodenum.
+
mtkilimanjaro
I think 2nd part of duodenum could be viable if the ampulla was not an option. The ampulla is way more localized/specific to this scenario
+2
sympathetikey
Short time course & tenderness was a tip for me.
+14
rainlad
Aka de Quervain's thyroiditis
+
karljeon
Can anyone explain why the serum lactate dehydrogenase (LDH) level was elevated?
+
asapdoc
Vitamin E is an antioxidant. Thus a deficiency can cause hemolytic anemia.
+6
sympathetikey
@karljeon Intravascular hemolysis = LDH release from RBCs
+4
dr.xx
loonies love lunate
+2
wes79
she landed on her "right hand", but the X-ray is showing a left hand??
+1
wes79
i legit have no idea whats going on in that xray lol
+11
nbme4unme
X-ray confused the hell out of me, I was going to put lunate based on Q stem but ended up putting Pisiform because it looks like that's what's messed up in the photo? Should have ignored the picture haha.
+1
nwinkelmann
for @dr.xx, love your mnemonic. I added to it, or at least found an explanation on why it works. "loonies love lunate" and "loonies" are "dislocated" from reality.
+3
niboonsh
Some Lovers Try Positions That They Cant Handle
+13
vsn001
ngl if scaphoid was an option - would've sprung at that real quick -> thanks for teaching me the importance of knowing to look for dislocation vs fracture :D
+
regularstudent
Ahh, the classic "left hand" x-ray but actual fracture of "right hand" NBME tactic
+
sars
I think the x-ray is showing the lunate protruding out of the palmar side. Imagine the situation where you are falling and using your hand to stop the fall. Your lunate will dislocate forward as the rest of the carpal bones recoil back, hence why it protrudes through the palmar side. Thats why it causes an acute carpal tunnel syndrome.
+
makingstrides
Another mnemonic, Some Lovers Tried Positions, That They Can't Handle
+
srmtn
in an X Ray (unless is marked) you can not know if is left or right.
this is a lunate dislocation but actually is dorsal...even though they put in the stem that is anterior... please google "gilula lines" in order to fastly check a wrist X-ray and find a dislocation... also I think that a good clue when wrist trauma is: dislocation is usually lunate and necrosis is usually scaphoid. hope it helps
+
sympathetikey
Probably in part due to early age presentation, but I hear you
+5
wowo
FA2019 p518 - process of elim for other spinal cord lesions
+2
cbreland
Also syringomyelia wouldn't have a position sense issue
+
gonyyong
Lol I guessed it exactly because of that
+8
karthvee
This is not prosopagnosia, but instead a case of apperceptive agnosia.
Wiki: "...patients are more effective at naming two attributes from a single object than they are able to name one attribute on each of the two superimposed objects. In addition they are still able to describe objects in detail and recognize objects by touch."
Although, lesions tend to be in the occipito-parietal area so PCA again is the answer!
+3
misterdoctor69
I actually think it's both prosopagnosia AND apperceptive agnosia. She is neither able to recognize her mother's FACE nor is she able to recognize objects w/o the help of other senses (apperceptive agnosia)
+2
nifty95
Yea couldn't remember the exact name but I just thought of three pathways (visual, somatosensation, and auditory) all converging somewhere/processor (probably somewhere in the temporal lobe...hippocampus?). Beyond the point, the pathways converge to an area which culminates in recognition.
Cut off one of the routes (in this case visual), the other two will still work. How is visual cut off? By the PCA not supplying the area leading to neuronal death resulting in varying loss of visual function depending on the area in the occipital lobe.
+1
zoggybiscuits
I thought it was spleen but the fact that hematocrit was 24% 4 HOURs later made me think otherwise. It was my understanding that the spleen would bleed you out quick!
+1
need_answers
couldn't also be ruptured spleen because they said intraperitoneal fluid and everything else is retroperitoneal ??
+4
peqmd
Spleen is most commonly ruptured in blunt trauma so along with myelofibrosis and being kicked on the left side it's just asking to be ruptured
+3
limberry
@need_answers the bladder is intraperitoneal, not retro
+
limberry
bladder is sub*peritoneal, sorry
+
sympathetikey
First off, do yourself a favor and check this out - https://www.youtube.com/watch?v=NJYNf-Jcclo
The LDL receptor is found on peripheral tissues. It recognizes B100 on LDL, IDL, and VLDL (secreted from the liver). Therefore, an issue with that would cause an increase in those, but mainly LDL.
Since in this question we see that Triglycerides and Chylomicrons are elevated, that points towards a different problem. That problem is in the Lipoprotein Lipase receptor. This is the receptor that allows tissues to degrade TGs in Chylomicrons. So, if it's not working, you get increased TGs and Chylomicrons. Additionally, you get eruptive xanthomas, which are the yellow white papules the question refers to.
+12
davidw
There is much easier way go to page 94 in first aid. This kid has Type 1 Hyper-Chylomicronemia which is I) Increased Chylomicrons, Increase TG and Increased Cholesterol.
It can be either Lipoprotein Lipase or Apolipoprotein CII Deficiency
+12
bulgaine
The video sympathetikey referred to only mentions pancreatitis in type IV but according to page 94 of FA 2019 it is also present in type I Hyper-chylomicronemia which is what the question stem is referring to with the abdominal pain, vomiting and increased amylase activity
+
dentist
thats not the only difference in that video....
+
paulkarr
Pixorize has a set of videos on all the lipid disorders that made it a breeze to answer.
Pixorize is basically sketchy but for biochem and other basic science subjects.
+3
futurelatinadr
Pancreatitis was a huge clue for me to think of hyperchylomicronemia
+1
sympathetikey
Agreed. I'm pissed though because PGE2 mediates pain, which is why I picked it.
+46
he.sanchez14
If im not mistaken, the question describes unstable angina. Unstable angina is due to thrombosis with incomplete occlusion. So, yes TXA2 is responsible for the thrombus that is causing the symptoms in this patient. I'm also pissed because I also went straight for the PGE2
+5
vik
hahah, seems like all in same boat like me
+
yb_26
thromboxane A2 is also vasoconstrictor, so my thoughts were about vasospastic angina
+8
need_answers
I went for leukotriene B4, what the hell was I doing....SHIT
+15
hopsalong
I picked Leukotrine B4 thinking that the neutrophil infiltration was the source of the pain, seems wrong lol.
+
bballhandler11
Sometimes it helps me to think of it in a general, non med school textbook kind of way. When answering, I narrowed it down to PGE2 and TXA2 as well. Then I asked myself, if someone is experiencing chest pain, would I recommend Aspirin or Advil? That's helped on a few over the counter pharm questions.
+12
ususmle
same here I M PISSED PGE2
+3
krewfoo99
Maybe PGE2 isint the answer because it mediates pain and fever during episodes of acute inflammation? Thus making TXA2 more likely.
+3
djtallahassee
ditto on the looked at it for 2 seconds and went PGE2
+1
veryhungrycaterpillar
My knee jerk reaction was to go with PGE2 for pain was well, but we must not forget that PGE2 is also a direct vasodilator. It also inhibits platelet aggregation.
+
kungfupanda
I'm on a whole new level. i thought this might be an asthma attack and i choose LTB4
+2
an1
Intermittent chest pain does seem like angina. E2 does cause pain, but it also causes fEvEr. TXA2 inhibits platelets (unstable) AND increases vascular tone (prinzmetal) which makes it a better option. E2 increases uterine tone (check sketchy), not vascular so it can be chosen if they were to mention labor.
+
meningitis
Could you elaborate? Is this related to: less "preload" from mother circulation causes lowered HR?
+
meningitis
Or backflow of blood and causes a Reflex Bradycardia? still confused on this question.
+
kentuckyfan
So I think the subtle difference in choice E is that there would be a negative CHRONOTROPIC effect, no inotropic effect (contractility).
+10
maxillarythirdmolar
if anything, inotrophy could go UP not down as diastole prolongs and LVEDV increases --> Starling equation bullshit
+
methylased
GATC related to methylase --> https://en.wikipedia.org/wiki/Dam_methylase
+10
zelderonmorningstar
Okay I feel like an idiot cause I thought: Above the Standard = Doing a good job keeping old people from getting ulcers. Thumbs up. Below the Standard = I wouldn’t let my worst enemy into your ulcer ridden elder abuse shack.
+68
aladar50
@zelderon Ohh damn. I could totally see how one could view the answer choices that way. I think it is important to read how they are phrased - they are asking if the center is above THE standard or below THE standard. The “standard” is an arbitrary set point, and the results of the study are either above or below that cut off. Maybe if it was “above/below standards” that would work. Also, being above the standard could either be a good thing or bad thing. If say you were talking about qualifying for a competition and you have to do 50 push ups in a minute, then being above=good and below=bad. In this case, having more ulcers than the standard = bad.
+4
saynomore
@aladar Thank you!!! but how did you get the 15 new ulcers per 180 patient⋅years? I mean I understand the 15 part, but not the second part ... hence why I messed this up, lol :|
+2
aladar50
@saysomore Because the study is looking at 100 residents over a period of 2 years. Since 10 already had the disease at the start, when looking at incidence you only include the subjects that have /the potential/ of developing the disease, so 90 patients over 2 years. This would be 90 patient⋅years per year, or a total of 180 patient⋅years over the course of the study.
+7
sympathetikey
@zelderonmorningstar I thought the same exact thing. Had the right logic, but then just put the backwards answer.
+4
kai
I wonder if they chose this wording on purpose just to fuck with us or if this was accidental. My guess is there's some evil doctor twirling his thumbs somewhere thinking you guys are below the standard.
+16
symptomatology
Got it wrong!messed up in understanding options,
Btw, 15/90 is somewhat 16 percent and their standerd is 50/1000 5 percent!.. this is how i knew that incidance is way up!
+
donttrustmyanswers
Patients with an ulcer are not immune to getting new ulcers --> You should include all patients at risk. But either way, the answer is the same as long as you can read NBME speak.
+
doublethinker
Damn, guess my reading comprehension is not "up to the standard" of the NBME writers. Smh.
+
prolific_pygophilic
If you forgot that its patient years (15/180) not (15/90) you still get the right answer because they are both above 5% :).
+
hpkrazydesi
Excess carotene in what way? sorry if thats a stupid question
+
davidw
this is directly from Goljan
"Dietary β-carotenes and retinol esters are sources of retinol. β-carotenes are converted into retinol. (a) Increased β-carotenes in the diet cause the skin to turn yellow (hypercarotenemia). Sclera remains white, whereas in jaundice the sclera is yellow, which can be used to distinguish the two conditions. (c) Vitamin toxicity does not occur with an increase in serum carotene"
+8
davidw
β-Carotenes are present in dark-green and yellow vegetables.
+1
dashou19
When I was a little kid, I like to eat oranges, like I could eat 10 oranges at once, and after a few days, I could tell that I turned yellow...
+8
cbreland
I'm okay with missing this one
+4
veryhungrycaterpillar
That was fucking stupid. I've known this excess carotene fact since 8th grade due to a friend getting it, but I still wouldn't have thought of it. I went with anemia, figured it had to be folic acid since B6 would have shown up sooner than four years. UGH.
+
an1
Vitamin C def would not occur in vegans and would cause scurvy symptoms. Folic Acid is HIGH in green leafy vegetables, We can assume vegans eat a lot of veggies. As this causes a megaloblastic anemia, the sclera would be expected to be pale. IFN a + ribavirin is used for hep, which is ruled out because of the normal urine and stool, and lack of scleral icterus. B1 def presents with wernickes/ Korsakoff often with excess alcohol intake and hypoglycemia uncorrected after dextrose. B6 presents with sideroblastic anemia + peripheral neuropathy (remember that INH caused B6 to be excreted resulting in neuropathy).
I got this wrong. Because who has time to go through every option and think it through, and who thought carrots would make the cut for this test.
+1
sympathetikey
Source: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/case-series
+2
ngman
I think another factor is that in case series studies there is no control group vs case-control, cohort...ect
+21
j44n
you dont need a control group in a cross sectional one so how do you differentiate that
+
imatinib2412
The key to eliminate cross-sectional study here is the "During a 5-year period" part; cross-sectional studies you basically "take a picture" of a certain population and evaluate prevalence of disease/risk factors at that point in time
+1
xxabi
Just to add - patient likely has MEN 2A or 2B with the presence of medullary thyroid cancer and pheochromocytoma
+14
dermgirl
The patient have MEN 2B (Medullary thyroid carcinoma + Pheochromocytoma) Page 351 FA.
+
sympathetikey
SeN Out (Snout) --> sensitive test; - test rules out
SPec In (Specin) --> specific test; + test rules in
+27
usmlecrasher
can anyone pls explain why it is not << potential false- positive results >> ???
+1
almondbreeze
correct me if I'm wrong, but 'high FP (choice C)=low specificity (choice B)'. Whereas high specificity is required to rule in dz
+2
almondbreeze
picked positive predictive value myself. can anyone explain why not PPV?
+1
williamfreakingosler
The principle @hayayah is talking about (a negative test being relied upon to reliably rule out) is negative predictive value ("NPV"). I don't see why "uncertain NPV" isn't the correct answer, particularly because NPV is predicated on the disease having the same base rate in the person(s) being tested as in the population that was characterized for the test statistic. Given that the patient has a strong family history of colon cancer, the NPV of FOBT is uncertain. Said another way, the sensitivity of a test does not change with the population, but the NPV does. The whole reason the doctor is denying FOBT is because of bayesian thinking (a priori information related to family history), and from my point of view bayesian logic is more relevant to PPV/NPV than to sensitivity, hence my confusion over why NPV isn't the right answer.
+4
ibestalkinyo
I thought negative predictive value for the same reasoning
+
raga7
AFTER THE RESULT OF TEST WE CAN USED PPV OR PPN, BUT FOR TEH FIRST TIME LOOKING ANY DESEASE USE SENSITIVITY OR SPECIFICITY.
+2
neonem
I think the best way to answer this question was by process of elimination.
+1
karljeon
Haha I eliminated the answer by process of elimination.
+25
medschul
I eliminated thiazides by process of elimination :(
+3
medstudent65
Shit I eliminated thiazides because of elimination went with HTN thinking intercranial bleed effecting the pituitary
+2
sympathetikey
Except according to FA, it's 68% within 1 SD, so 34%, which split in half is 17%.
+2
amirmullick3
Sympathetikey check your math :D
100-68 is 32 not 34, and half of 32 is 16 :)
+8
lilyo
Can anyone explain why we subtract 68 from 100? This makes me think that we are saying its 35% of the data that falls within 1SD as opposed to 65. HELLLLLLP
+
sallz
@Lilyo If you consider 1 SD, that includes 68% of the population (in this case, you're saying that 68% of the people are between 296 and 196 (1SD above and 1 below). This leaves how many people? 32% outside of that range (100-68=32); half of those would be above 296 and the other half below 296, so 16%
+5
sympathetikey
Correct. Per first aid: "If the 95% CI for odds ratio or relative risk
includes 1, H0 is not rejected."
+2
xxabi
Ah that makes more sense, thanks!
+
drdanielr
Since the OR or RR is a ratio, if the two interventions are equal the ratio would be 1. So, if the CI includes 1, they are "the same" or not stat sig diff
+
ergogenic22
Meckel diverticulum also occurs distal to the CBD but less likely to be associated with bilious vomiting
+
sympathetikey
Correct. Might cause pain due to ectopic gastic tissue.
+3
sympathetikey
Same. Learn something new every day:
See more: https://www.fda.gov/safety/medwatch-fda-safety-information-and-adverse-event-reporting-program
+5
karljeon
I didn't choose it because it was so damn specific. :(
+48
lovebug
Could anyone explain for B) for me? because I choose B).:(
+2
j44n
B.) is wrong because its never been shown to show adverse effects "any offcial data linking the drug" and the fact that it's "newly marketed"
+
j44n
and because its in 5/45 patients roughly 10% of the population, that might not seem like much but most of the diseases we freak out over are in 1-2% of the population, to put that into perspective if we gave this drug to every person in the US (every big pharma wet dream) with a population of 300 million... 30 million people would have this adverse event... hope that helps
+
thepacksurvives
I think that there can also be a direct tear to the anal sphincter muscles
+8
sympathetikey
A better answer choice would have been "damage to the nerves innervating the anal sphincter" but eh, ok.
+22
nerdstewiegriffin
I it is due to actual tear of external and or internal anal sphincter
Source uptodate
+2
sympathetikey
Yeah, I was thinking about that while taking the exam. Just got thrown off because I don't see how that matters, now that they've fractured the femur. How do prior increases in bone density allow for better chances of bone healing?
+19
rsp
I think that bone density is important here, but think about all of the other things that go in to recovering from a fracture at that age too. How strong are the muscle that will stabilize you while going through the motions of physical therapy? How conditioned are you?
+4
j123
I'd put money on a fat baby who doesn't exercise to heal faster than my 95 yo grandpa who rides his stationary bike 2 hrs per day... lol
+1
stresssweat
In that same train of thought, another modifiable risk factor for fracture would be levels of calcium and vitamin D intake throughout childhood. I crossed these out because they were essentially the same thing so obviously neither could be right, but aside from that - what would be the actual reason those were wrong?
+
medschul
Would pheo have a normal resting BP though?
+16
meningitis
I was trying to justify these tricky questions but very true medschul.. It shouldn't have normal resting BP. Sometimes it seems these NBME always have a trick up their sleeve. Im getting paranoid lol
+
nala_ula
The reason why the patient probably has normal HTN is because Pheochromocytoma has symptoms that occurs in "spells" - they come and go. Apparently in that moment, when the physician is examining her, she doesn't have the HTN, but like @meningitis explained, so many adrenergic hormones around leads to double the vasoconstriction when the patient stands up.
+10
meningitis
Thank you @nala_ula for your contribution! Really filled in the gap Iwas missing.
+2
nala_ula
No problem! Thank you for all your contributions throughout this page!
+2
mjmejora
I thought the pheochromocytoma was getting squeezed during sitting and releasing the epinephrine then. kinda like how it can happen during manipulation during surgery. Got it right for sorta wrong reasons then oh well.
+
llamastep1
When she sits in the examination table there would be a normal activation of the sympathetic system from the stress of getting examined which is amplified by the pheo. Cheers.
+
sammyj98
UpToDate: Approximately one-half have paroxysmal hypertension; most of the rest have either primary hypertension (formerly called "essential" hypertension) or normal blood pressure.
+
notyasupreme
Damn llama, that is WAYYY too much of an inference. Maybe if they said she was nervous in general or something, but not everyone gets stressed out by a doctor hahaha
+
jakelong377
It’s not about being stressed infront of doctor. When u stand sympathetics activate to prevent orthostatic hypotension, to counter it adrenal medulla released catecholamines so much so that pheochromocytoma patients would appears with flushed skin n such
+
sympathetikey
Yes, but doesn't that mean maternal transmission? Men can have these diseases too, they just won't pass them on.
+32
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The whole "picks at the lesion...causes some bleeding", made me think Psoriasis. Should have gone with Actinic Keratosis based on the patient history (lots of sun exposure).
Actinic Keratosis
Premalignant lesions caused by sun exposure. Small, rough, erythematous or brownish papules or plaques. Risk of squamous cell carcinoma is proportional to degree of epithelial dysplasia.