First question : They tell us its a lymphocytic leukemia
Second question : Deciphering whether it is a B cell or T cell.
The cells have no surface bound Ig M ,Ig G or cytoplasmic chains for these antibodies , but have a rearranged gene segment( meaning active ) for the T cell Receptor . So the Cells are T Cells
Third question : Now that we know that they are T Cells , we want to know whether they are CD4 or CD 8 positive
The cells in the clinical vignette lack both CD4 and CD 8 ( double negative )
According to how T cells normally develop - They start of as being double negative ( i.e not expressing CD4 or CD 8) in the subcapsular region and progressively become
- positive for both CD 4 and CD 8 in the cortex
- and eventually acquire the TCR and CD3 by the time they get to the medulla
These cells therefore must T lymphocyte thymocytes localised to the cortex
Posterior cord syndrome occurs due to infarction of the posterior half of the spinal cord, from occlusion of the posterior spinal artery. Our patient presents with decreased sensation to pinprick below the level of the knees as well as walking with a wide-based gait, likely indicating loss of proprioception. The patient is also anemic with hyper-segmented neutrophils.
Hypersegmented neutrophils are typically caused by an inability to make enough DNA, caused by a lack of necessary precursors and vitamins including B9 (folate) and B12 (cobalamin). If the patient is folate deficient, we see elevated homocysteine deficiency. If the patient is B12 deficient, we see elevated methylmalonic acid and homocysteine levels. Hyperhomocysteinemia can increase thrombosis. Thrombosis in the posterior spinal artery can cause posterior cord syndrome. In addition, lack of vitamin B12 impairs myelin formation and leads to Subacute Combined Degeneration, which affects the Spinothalamic tract (accounting for decreased pinprick sensation), Corticospinal Tract, and Dorsal Column-Medial Lemniscus Tract (accounting for the reduced proprioception.
A) Anterior cord syndrome- loss of motor command, as well as bilateral loss of heat and pain, the patient has not lost motor function, so it cannot be this. B) Central cord syndrome- presents as a combination of motor and sensory loss, usually with bladder dysfunction. This patient does not display motor loss or bladder dysfunction. C) Hemicord syndrome- Also called Brown-Sequard, this is complete injury to either the left or right side of the spinal cord. It presents with motor dysfunction and reflex dysfunction ipsilaterally at the level of the lesion; loss of upper motor command below the lesion ipsilaterally (spastic paresis); loss of dorsal column-carried sensation ipsilaterally at and below the lesion; and loss of pain and temperature sensation contralaterally 2 to 3 vertebra below the lesion. E) Segmentary syndrome- a congenital failure to develop part of the spinal cord. The new onset of symptoms at 82 years old makes this an unlikely diagnosis,.
Lucky deduction, but looking back, I believe what they were going for is what she should have been vaccinated for at 6 months of age (since there are no apparent symptoms).
Hep B vaccine is usually given at birth, 1 month, and 6 months of age, so it's pretty important that she be vaccinated against it, unless she already has it, in which case she should be treated to avoid cirrhosis.
I actually think I found the exact same image in color and fully labeled... and VIII is labeled as C here... https://d1yboe6750e2cu.cloudfront.net/i/c8494948ed5e0460ae33c5ecb6be887208f9d8c1
I tried to use logic to answer this question (I did not know about the hexosamine pathway). Here is my attempt--this is probably wrong somewhere.
I figured that if you want to make glucosamine, you need to combine glucose + an amine group
(A) Arginine I knew was involved in donating nitrogen, but it is in the urea cycle, so I figured this was probably not the answer but it had potential. I figured that the major way this compound removes its nitrogen is through urea, though.
(B) ATP. Since F6P already has the phosphate group, I figured ATP is probably not necessary as the compound in question already has a PO4 group.
(C) Carbamoyl phosphate. I knew this was involved in both the urea cycle and nucleoside synthesis, so this was less likely. It also is the product of a NH3 and CO2 so that means that I wouldn't expect it to donate an amine group
(D) Glutamine I figured has an amine group attached to it ready for donation. I also know that transamination reactions are common with amino acids and alpha-ketoacids (e.g. alpha ketoglutarate with alanine can get you glutamate and a pyruvate via ALT) thus it made sense that an amino acid could donate an amine group.
(E) The only thing I knew about NAG was that it was used in the urea cycle as an allosteric activator of CPS, so I didn't think that it was useful as a donator of nitrogen since its function is to help aid nitrogen excretion.
So then I was stuck between A and D, but based on transamination reactions, I picked D.
Hyperparathyroidism causing bone lesions is via Osteoblasts increasing RANK -L expression to bind to RANK on Osteoclasts and stimulating them ---> inc Bone Resorption
Niacin (vitamin B3) antagonizes VLDL cholesterol secretion
I was so fixated on the fact that in a TB granuloma, macrophages produce IL12 or TNFalpha, not IL1. So I eliminated C and clicked B, even tho it’s not CD4 lymphocytes that produce TNFalpha. But the fact that macrophages produce IL1 still didn’t make any sense.
I couldn’t find any explanation in first aid for this (it doesn’t tell you what cells secrete IL1), but according to my notes from an immuno lecture I half paid attention to, IL1 is a cytokine of innate immunity secreted by monocytes, macrophages, endothelial cells, and epithelial cells; so basically everybody. This goes in conjunction with everything that FA says (FA18 p. 108)
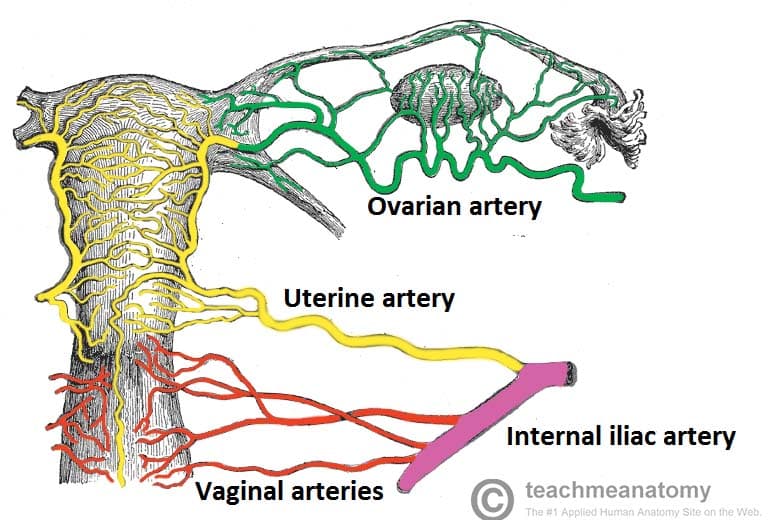
My thought process was that post-partum bleeding is usually related to the uterus, and much of the pelvic viscera is supplied by branches of the internal iliac artery.
You're just going to diss the son like that right in front of him?
what to do with the NONADHERIANT BADDIES???
Intention to treat, "i had the intention to treat so i am gonna leave in this group no matter what"
as treated , "he is not treated as it is so im gonna change his group to control"
per protocol, "you are fired from all of it, protocols bitch"
You would think the rectus femoris is in the back bc rectum, and biceps is in the front. But no. Okay then.
Can anyone explain why the lipase concentration is so high if there is an issue with LPL in hyperchylomicronemia?
A radiographically visible air-fluid level suggests a pretty large lesion (hence, “cavitary”). That's not going to become normal tissue again. Six months following resolution of symptoms you can expect healing in the form of a scar; that is, fibrosis but only in a single spot.
Neoplasia is new tissue growth that is unregulated, irreversible, and monoclonal.
Clonality can be determined by glucose-6-phosphate dehydrogenase (G6PD) enzyme isoforms. G6PD is X-linked.
*For more information check out Ch. 3 Neoplasia in Pathoma
Defective homologous recombination is seen in breast/ovarian cancers with the BRCA1 gene mutation.
Falling on outstretched hand: scaphoid is most common one to be fractured, lunate is most common to be dislocated. Lunate dislocation can cause acute carpal tunnel syndrome.
Think of the mnemonic "Straight Line To Pinky, Here Comes The Thumb" for the bones of the palm, drawing a football shape starting below the thumb MCP joint adjacent to the radius, then moving to your medial wrist, and then back to the thumb.
Scaphoid, lunate, triquetrum, pisiform, hamate, capitate, trapezoid, trapezium. The lunate looks like it's posteriorly dislocated here.
Case-series: comparing patients with a KNOWN OUTCOME (disease) to others with the same disease and looking back to see if they were exposed... "Did 2 people with the same disease get it from the same place?"
Case-control: comparing patients with a KNOWN OUTCOME (disease) to others WITHOUT (control) the disease and looking back to see if they were exposed. (odds ratio)... "they are sick and you want to see if drinking the contaminated water caused it by comparing them to normal people."
Cohort: Comparing patients with a KNOWN EXPOSURE and moving forward with them (prospective) or looking back in time (retrospective) to see if they developed the outcome (disease). (relative risk)... "they all drank the contaminated water and you want to see if they are more likely to get the disease."
Correlation is a statistical analysis used when both the dependent and independent variables have quantitative measurement values.
I hope this is right and helps... :)
This patient has a pneumothorax. Hyperventillation is not enough to compensate for the overall decrease in lung surface area.
Androgen Insensitivity Syndrome - Defect in androgen receptor resulting in normal-appearing female (46,XY DSD). Functioning testes causes increased testosterone at puberty, which is converted to estrogen peripherally, giving female secondary sexual characteristics (female external genitalia). Lack of androgen receptor function leads to absent or scant axillary and pubic hair. Patients have rudimentary vagina, but uterus and fallopian tubes absent.
Androgen insensitivity syndrome is the answer but you might have considered Müllerian agenesis (Mayer-Rokitansky- Küster-Hauser syndrome).
Mullerian agenesis will have normal hormone levels and may present as 1° amenorrhea (due to a lack of uterine development) in females with fully developed 2° sexual characteristics (functional ovaries). Hair development is normal as well. Patients also have normal height.
Seems like this question did not give us much to distinguish besides height and tanner stage 1 pubic/axillary hair.
Androgen Insensitivity Syndrome - Defect in androgen receptor resulting in normal-appearing female (46,XY DSD). Functioning testes causes increased testosterone at puberty, which is converted to estrogen peripherally, giving female secondary sexual characteristics (female external genitalia). Lack of androgen receptor function leads to absent or scant axillary and pubic hair. Patients have rudimentary vagina, but uterus and fallopian tubes absent.
Androgen insensitivity syndrome is the answer but you might have considered Müllerian agenesis (Mayer-Rokitansky- Küster-Hauser syndrome).
Mullerian agenesis will have normal hormone levels and may present as 1° amenorrhea (due to a lack of uterine development) in females with fully developed 2° sexual characteristics (functional ovaries). Hair development is normal as well. Patients also have normal height.
Seems like this question did not give us much to distinguish besides height and tanner stage 1 pubic/axillary hair.
Why there's no increase in Hydrostatic pressure in glomerular capillaries?
{kind=link}
{kind=link}
On top of the previous post, migraines last for 4+ hours. and Tension headaches are bilateral.