Contributor score: 110
at my uni, we learnt that at lower GFR, loop diuretics still work. That's why you should use them in renal failure. Thiazides would not work with a GFR of <30.
This is a picture of Giardia lamblia… caused by drinking contaminated water with cysts.
Multinucleated trophozoites
Rx -- Metronidazole -- forms toxic free radical metabolites in the bacterial cell that damage DNA = BACTERICIDAL
The Didanosine guy in the NRTI sketch is holding a pancreas sponge.
Membranous Glomerulonephritis is Nephrotic; ONLY PROTEINURIA is in the vignette
It can't be MPGN because MPGN is Nephritic with possible Nephrotic
Other choices are eliminated by Renal Biopsy
The synthesis of virtually all proteins (mRNA->peptide) occurs in the cytoplasm.[1] That’s where all ribosomes reside, after all. Ribosomes, which are mostly just rRNA (~2/3 rRNA + 1/3 protein*, by weight), are assembled in the nucleus but only do their stuff once they get to the cytoplasm.
For a protein to leave its original hometown of the cytosol and become a resident of the nucleus or, say, the endoplasmic reticulum, it needs to have a little string of amino acids which shout “I belong in the nucleus!” or “I belong in the endoplasmic reticulum!”
Proteins ultimately destined for the ER contain an unimaginatively named string of amino acids known as “signal sequence,” which, for the purposes of the Step 1, is always at the N-terminus. The signal sequence tells other cytosolic proteins, “Hey! Take me (and the rest of the peptide of which I am part) to the ER!”
In the absence of this signal, a protein will remain in its “default” home of the cytosol.
Here’s a nice schematic showing the flow of proteins from initial synthesis to final destinations:
Endnotes
- “The synthesis of virtually all proteins in the cell begins on ribosomes in the cytosol.” (Essential Cell Biology, Alberts et al., 2014, p. 492)
*If you really want your mind blown, consider that even the protein subunits that make up that 1/3 of a ribosome are themselves initially synthesized in the cytosol; later, they are transported back into the nucleus via the nuclear pore.
the majority of carbon dioxide molecules are carried as part of the bicarbonate buffer system. In this system, carbon dioxide diffuses into the RBCs. Carbonic anhydrase (CA) within RBCs quickly converts the carbon dioxide into carbonic acid (H2CO3). Carbonic acid is an unstable intermediate molecule that immediately dissociates into bicarbonate ions (HCO3-) and hydrogen (H+) ions.
The newly synthesized bicarbonate ion is transported out of the RBC into the plasma in exchange for a chloride ion (Cl−); this is called the chloride shift. When the blood reaches the lungs, the bicarbonate ion is transported back into the RBC in exchange for the chloride ion. The H+ ion dissociates from the hemoglobin and binds to the bicarbonate ion. This produces the carbonic acid intermediate, which is converted back into carbon dioxide through the enzymatic action of CA. The carbon dioxide produced is expelled through the lungs during exhalation.
{kind=link}
It said it was fatal to males in utero, and the question asked about live born offspring. Since the males aren’t being born in the first place, I said 50% females and 0% males.
Rabies Virus (rhabdoviridae)
Fever, encephalitis, drooling
HELLP syndrome: Hemolysis Elevated Liver enzymes Low Platelets.
A manifestation of severe preeclampsia. Blood smear shows schistocytes. Can lead to DIC and hepatic subcapsular hematomas rupture severe hypotension.
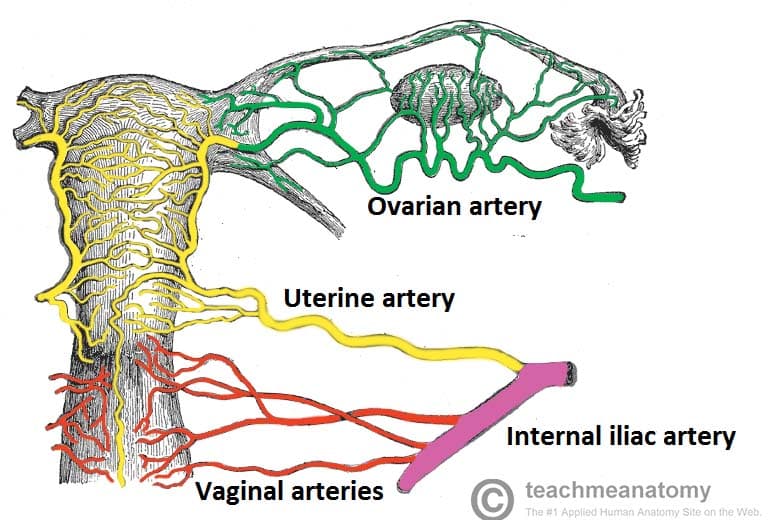
https://teachmeanatomy.info/wp-content/uploads/Blood-Supply-to-Female-Reproductive-Tract.jpg
{kind=link}
- APocrine = your armpits smell like an APE
- ceRUMen = there’s no ROOM in your ears since they’re full of wax
- EC-CRYne = when you ECercise, your pores are CRYing
- SEBaceous = SEBum is SEEPing out of your pores
Rosacea. An inflammatory facial skin disorder characterized by erythematous papules and pustule but no comedones. May be associated with facial flushing in response to external stimuli (eg, alcohol, heat).
{kind=link}
The puborectalis muscle, which is one of the muscles that comprise the pelvic floor and plays an important role in both fecal continence and defecation, is tonically contracted and maintains the anorectal angle at rest.
here is a picture: https://www.123rf.com/photo_46940875_stock-vector-the-rectum-and-anus-showing-the-puborectalis-muscle-part-of-the-levator-ani-used-for-the-control-of-.html
In an elderly patient with isolated elevated alkaline phosphatase (normal serum calcium and phosphate) Paget's disease of bone should be at the top of the differential. This disease is due to dysregulation of osteoclastic and osteoblastic activity; first an initial osteoclast hyperactivity phase, then increased osteoblast activity for a mixture, then osteoclasts "burnout" leading to over-mineralization and sclerotic bone plaques. In addition, this can create arteriovenous shunts in the bones which decreases resistance, leading to high output cardiac failure (a similar problem can arise in arteriovenous fistulas from blood dialysis). On histology it will have a "mosaic" pattern.
A)- Aneurysmal bone cyst- largely a product of hyperactivity of osteoclasts, this occurs more often in the limbs, and shows a cystic space with balloon-like dilation. B) Angiosarcoma- angiosarcoma of the bone is n almost purely lytic lesion. They occur more frequently in younger people. C) Niacin deficiency- I can find nothing about vitaminb B3 deficiency involving bones. B3 deficienct results in pellagra, with the classic Three D's- dermatitis (rash necklace on C3/C4 dermatome), dementia, and diarrhea. E) Osteosarcoma- Found almost exclusively in younger people, this bone growth occurs at the growth plate, particularly at the proximal end of the tibia, distal end of the femur, or proximal end of the humerus (in the long bones around your knees or at your shoulders). It shows a large, solid growing mass that may raise the periosteum in a sunburst pattern/Codman's triangle. F) Prostatic carcinoma- rare for being one of, if not the only metastatic bone cancer that is purely osteoblastic.
"His friends believe there may have been drugs at the party", period. lmao...
So for Candida we can use
Azoles (fluconazole) (inhibit CYP450 demethylation)
Amphotercin B (pore formation in fungal cell membrane)
Caspofungin (prevent crosslinking of beta glucans in cell wall)
or Nysatin for oral or esophageal cases (pore formation)
This question is saying that she is taking an ORAL drug to treat candida vaginitis.
Amphotercin is IV
Caspofungin is also IV
so we're left with azoles
Azoles inhibit synthesis of ergosterol by inhibiting CYP 450 that converts lanosterol to ergosterol.
Maintenance dose formula is (Css × Cl × tau) ÷ F
where Css is steady-state target plasma conc. of drug, Cl is clearance, tau is dosage interval & F is bioavailability.
Neither dosage interval nor bioavailability is given, so ignoring those & plugging in the numbers (careful to convert units to mg/kg/day):
=(12 ug/mL × 1 mg/1000 ug) × (0.09 L/hr/kg × 1000 mL/1 L × 24 hr/1 day)
= 25.92 mg/kg/day
...which isn't any of the answer choices listed. They must have rounded 0.09 L/hr/kg to 0.1 L/hr/kg, and doing so gives exactly 28.8 mg/kg/day (choice C)
{kind=link}
Believe this question is referring to Visceral Leishmaniasis.
It was a type IV HSN reaction, which deals with T cells and that was the only answer that had t cells involved.
A normoblast is an immature RBC, so it's elevated in states of increased hematopoiesis.
This patient presents with a small cell carcinoma which is very common for para neoplastic syndromes. In this case the cancer is causing SIADH. Demeclocyline is a tetracycline antibiotic that is also used to treat SIADH
my approach to this question was to eliminate all the answer choices that mentioned specificity or sensitivity, since the data here did not provide information about any sort of screening test.
that left me with two possible answer choices: I eliminated the one about consistency of other studies, since no other studies were mentioned in the question stem.
not sure if I oversimplified things, but it led me to the right answer!
"PV is a neoplastic (clonal) blood disorder with autonomous (EPO-independent) erythroid proliferation. Because of the existence of a negative feedback mechanism, the erthrocytosis in PV down-regulates EPO production and results in below normal serum EPO levels. In contrast, an EPO-driven erythrocytosis characterizes secondary erythrocytosis, and this condition may be associated with either high or normal serum EPO levels."
https://www.mayoclinicproceedings.org/article/S0025-6196(11)63840-8/fulltext
Cholera = Fecal oral /Legionnaires = Legonalla pneumo = NO person to person only by inhalation of bacteria contaminated water /Lyme = tick bite /Meningiococcal = sharing respiratory and throat secretions (saliva or spit). Generally, it takes close (for example, coughing or kissing) or lengthy contact to spread these bacteria (CDC) /RMSF = tick bite
Great video I used to learn this material.