In case anyone else was wondering about the other choices:
A: Acetyl-CoA carboxylase is the first committed step in fatty acid synthesis
B: Homocysteine methyltransferase turns homocysteine into methionine (we can deduce this from knowledge about homocystinuria)
C: Methionine adenosyltransferase makes SAM. SAM has two roles that we know of - one in turning methionine back into homocysteine, and one turning norepinephrine into epinephrine. This could make it a tempting choice but at the time I just saw the word 'methionine' and thought that couldn't have anything to do with cortisol/catecholamines.
D: LOL for methylmalonyl-CoA racemase, wiki says "It is routinely and incorrectly labeled as 'methylmalonyl-CoA racemase'. It is not a racemase because the CoA moiety has 5 other stereocenters." Good job NBME. Anyway, methylmalonyl-CoA epimerase is involved in the same catabolic pathway that we know of through propionic acidemia, so it's involved in breakdown of fatty acids and amino acids.
Here my stab at summarizing all the info. The first diagram on this website is a super helpful as well; This diagram sorta helps too.
Normally, bilirubin from the blood stream is conjugated in the liver to a water-soluble form. This gets mixed with bile to be excreted through the intestines. In the small intestine, it becomes urobilinogen, some of which is excreted by the kidneys, giving pee that good yellow color. Some of the urobilinogen turns into stercobilin and stays in the GI to be excreted in poop, giving poop that good brown color.
In bile duct obstruction, bilirubin gets conjugated to a water-soluble form - then it's stuck. It's unable to be excreted into the intestines, unable to turn into urobilinogen or stercobilin, etc. Conjugated bilirubin builds up in the liver, and eventually gets backed up back into the blood stream where it came from. Since it's water-soluble and floating around in circulation, it eventually gets filtered by the kidneys and ends up in pee. Bilirubin is darker in color, so the pee would be dark. However, the stool would be pale since no stercobilin was made. I believe that symptoms of itchy skin also occurs in these cases as bile salts back up and are deposited in skin.
Hemolysis is not the correct answer because most of the bilirubin is not yet conjugated, so it's not water-soluble and doesn't end up in the kidneys.
SPOILER ALERT!!
Do not read ahead if you have not taken NBME 22!!!
I'm smh at this question because in NBME 22, they describe a scenario in which loperamide caused CNS effects - particularly ventilatory depression and we were supposed to know that it was loperamide. I guess this question specified "little to no" rather than "none at all" but come ON, I'm annoyed that we have to separate such nitpicky detail when one question emphasizes its lack of CNS effects, then they turn around and test us on an exception of this exact same content. /end rant
This was not very informative at all, I just wanted to consolidate a similar question that I knew I had just seen but it turned into me just being angry I'm sorry.
I am for some reason learning about this for the first time so I'll write a bit about euthyroid sick syndrome in case it helps someone.
It's a disease of exclusion - the thyroid hormones are whack but the thyroid gland itself seems to be totally fine. Specifically, T3 levels are low, rT3 is high (the activity of different deiodinases are off, so rT3 is made more and degraded less, though it doesn't seem like the rT3 level has any other clinical implications). As the other comments have mentioned, TSH and T4 are typically normal, although they can be decreased as well in severe cases.
Euthyroid sick syndrome is typically due to an underlying critical illness or starvation - the body stops making the hormones as an extreme measure to save energy and resources. The treatment is to treat the underlying illness; thyroid hormone therapy is not recommended as its effectiveness is inconclusive.
In this question stem, the patient has an underlying illness. Her thyroid gland works fine (responds appropriately to TSH). Classic case of euthyroid sick syndrome.
Given that her T4 levels are normal, we can rule out B, D, and E. I'm a dumdum and put C because I had no idea what euthyroid sick syndrome was. But given that her TSH level is also normal, it's not an issue with the hypothalamus or pituitary gland.
(Sources: wiki page and this article)
Here is my summary of the picture/video that was posted:
There are 3 pathways involved in peeing:
Pelvic n. (aka pelvic splanchnic n.) sends parasympathetic fibers to deltrusor to contract --> squeeze bladder and pee.
Hypogastric n. sends sympathetic fibers to the deltrusor to relax, as well as the internal sphincter to contract --> hold back pee
Pudendal n. sends somatic fibers (under conscious control) to the external sphincter to contract --> hold back pee
In this question, the patient's bladder is filling up so much that it's forced to overflow. That means there is a problem with scenario 1 - damage to pelvic n. so that he can't squeeze his bladder even when it's super full.
While I understand why it's hyperplastic arteriosclerosis and how it classically occurs with HTN, I was wondering why it couldn't be berry aneurysm? Is it because the question is asking which is "most likely", making C the better answer? Thank you.
from @melchior
From the UW ID 666 explanation, although type II pneumocytes normally differentiate into type I pneumocytes after proliferation, they do not differentiate in idiopathic pulmonary fibrosis due to altered cell signals and altered basement membrane, which is why type II pneumocytes are increased.
explanation by @benwhite_dotcom is incorrect
Damn everyone out here looking at the eyes when my dumbass was thinking the girl was missing a nasal bridge or something lol fml
The analysis only showed a mutation in one allele. CF is an autosomal recessive disease: the disease only manifests if there are mutations in both alleles of the CFTR gene.
If you still have 1 functional copy of the CFTR gene, you can still make the CFTR protein (the chloride channel/transporter), hence your body won’t have any issues.
This is analogous to tumor suppressor genes like Rb: so long as one of the alleles you have is functional, you can make enough of the protein to “make up” for the defective allele. If both get knocked out (Rb-/-), you lose the protection provided by the gene because now you make no protein at all.
The only thing that made sense for this question was the fact that the other allele was not included in the analysis.
MHC class 1 peptide antigen processing > "Antigen peptides loaded onto MHC I in RER after delivery via TAP (transporter associated with antigen processing)" - First Aid 2019.
Bare lymphocyte syndrome type 2 (BLS II; affecting MHC II) is due to mutations in genes that code for transcription factors that normally regulate the expression (gene transcription) of the MHC II genes. Bare lymphocyte syndrome type 1 (BLS I; affecting MHC I), is much more rare, and is associated with TAP deficiencies.
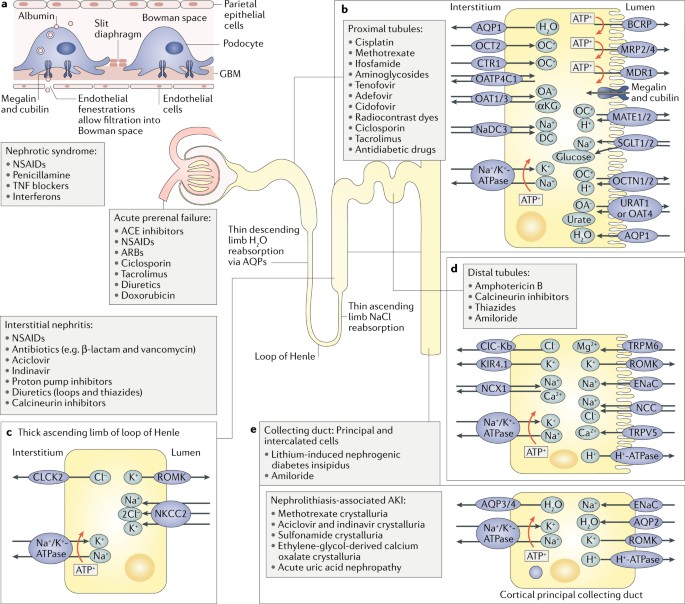
ATN ( Acute Tubular necrosis ) may be either ischemic or nephrotoxic:
*Toxic - tends to affect the PCT ( convoluted segment )
Aminoglycosides are nephrotoxic; nephrotoxic chemicals/drugs cause acute tubular necrosis (ATN), characterized by damage to the PCT. ATN causes the formation of brown, muddy, granular casts in the urine. The fact that this patient is a quadriplegic might be suggesting that they have a lower volume of distribution for the drug (and therefore higher blood concentrations).
SIADH is characterized by :
*Excessive free water retention ( less water in urine means specific gravity increases and not decreases as in option E)
*Euvolemic hyponatremia with continued urinary Na+ excretion ( and so urine Na which actually be greater than and not less than 10 mEq/L option D)
*Urine osmolality > serum osmolality ( option C)
Serum potassium does not actually decrease ( counter-intuitively ) because the excess fluid retention suppresses aldosterone secretion . The two main stimuli for potassium loss/secretion in kidneys are - aldosterone - and high urine flow rates. Both of these are decreased in SIADH ( excluding option B )
Serum urea nitrogen and creatinine are diluted , so their concentration decreases
In SIADH, the excessive ADH causes the collecting duct of the kidney to reabsorb huge amounts of water that it should normally excrete. That means that the plasma will now have much more water relative to solute (low osmolality) and the urine will have much more salt relative to water (higher osmolality).
Baby developed RDS --> guven O2 as Rx --> complications of O2 herapy in neonated = RIB (FA 2019) R = Retinopathy of prematurity I = Inraventricular hemorrhage B = Bronchopulmonary dysplasia
Baby developed RDS --> guven O2 as Rx --> complications of O2 herapy in neonated = RIB (FA 2019) R = Retinopathy of prematurity I = Inraventricular hemorrhage B = Bronchopulmonary dysplasia
Baby developed RDS --> guven O2 as Rx --> complications of O2 herapy in neonated = RIB (FA 2019) R = Retinopathy of prematurity I = Inraventricular hemorrhage B = Bronchopulmonary dysplasia
What of if the cancer is a urothelial cancer in the bladder due to radiation therapy. would it not cause similar signs
What of if the cancer is a urothelial cancer in the bladder due to radiation therapy. would it not cause similar signs
Loop diuretics are first line for acute congestive heart failure. That should help you remember that they are the most potent diuretics, so they're often used in the acute treatment of edema.
I was duped; did anybody here get it wrong because they thought about the thyroid ima artery arising from the brachiocephalic trunk? No? Just me? Okay.
"Since symptoms can increase in severity during the night, it could become difficult to fall asleep or return to sleep after waking up"
"RLS is one of several disorders that can cause exhaustion and daytime sleepiness, which can strongly affect mood, concentration, job and school performance, and personal relationships. Many people with RLS report they are often unable to concentrate, have impaired memory, or fail to accomplish daily tasks"
"RLS occurs in both men and women, although women are more likely to have it than men."
"the symptoms typically become more frequent and last longer with age".
Everything in the stem points towards restless leg syndrome.
Plus I thought you need 5/9 of the SIG E CAPS to diagnose depression.
Someone please explain :)
don't be a dick? not really sure what more there is to it. The patient doesn't have any other family so this woman should be considered family
The medical requirements to obtain a permit vary by state, but are usually confined to specific types of disabilities or conditions. These as a general rule include the use of any assistive device such as a wheelchair, crutches, or cane, as well as a missing leg or foot. Some states also include certain cardiovascular, pain, or respiratory conditions. About half of US states (26) include blindness as a qualifying disability enabling the person to obtain a disability parking permit for use as a passenger, and 14 states include a disabled hand as a qualifying disability. Four states include deafness, and two states (Virginia and New York) include mental illness or developmental disabilities as qualifying disabilities
our guy uses a cane so...
btw i got it wrong :) cause i thought it is up to the DMV
Answer E
Inorganic Phosphorus ; Parathyroid Hormone ; Calcitriol
Decreased ; Increased ; Decreased
This patient is suffering from celiac sprue, which in this case has caused Vitamin D malabsorption and therefore decreased serum calcium. The body will respond to the decreased calcium via secretion of PTH. This will then cause phosphorous wasting to occur in the proximal convoluted tubule.
According to the Nurses' Health Study, the risk of pulmonary adenocarcinoma increases substantially after a long duration of tobacco smoking: smokers with a previous smoking duration of 30–40 years are more than twice as likely to develop lung adenocarcinoma compared to never-smokers (relative risk of approximately 2.4); a duration of more than 40 years increases relative risk to 5.[8]
This cancer usually is seen peripherally in the lungs, as opposed to small cell lung cancer and squamous cell lung cancer, which both tend to be more centrally located,[9][10] although it may also occur as central lesions.[10] For unknown reasons, it often arises in relation to peripheral lung scars. The current theory is that the scar probably occurred secondary to the tumor, rather than causing the tumor.[10] The adenocarcinoma has an increased incidence in smokers, and is the most common type of lung cancer seen in non-smokers and women.[10] The peripheral location of adenocarcinoma in the lungs may be due to the use of filters in cigarettes which prevent the larger particles from entering the lung.[clarification needed][11][12] Deeper inhalation of cigarette smoke results in peripheral lesions that are often the case in adenocarcinomas of the lung. Generally, adenocarcinoma grows more slowly and forms smaller masses than the other subtypes.[10] However, it tends to metastasize at an early stage.[10]
other answer choices
black fly - onchocera volvulus (river blindness) tsetse fly - trypanosoma brucei (african sleepling sickness) deer fly - F. tularensis
so I don't think the reason for bilateral hydronephrosis is because it invated the bladder or kidneys. it is probably due to obstruction. there is a cancer in the uterine side of cervix (uterine cervix) that is big and its pushing on the bladder and its obstruction the flow of urine in ureters to bladder, so the urine backs up to the kidney and causes bilateral hydronephrosis and hydronephrosis. the kidney and ureters are full of urine and the cannot empty it to the bladder because this mass in the cervix is pushing on bladder and opening of ureters and squeezing bladder to the pubic bone.
Weight loss - think cancer Hyponatremia - SIADH from small cell lung cancer Edema + JVD - SVC syndrome
why not sarcoidosis? 1.rheumatoid arthritis like symptoms 2.uveitis 3.kidneys ...only serositis is a bit controversial
why not sarcoidosis? 1.rheumatoid arthritis like symptoms 2.uveitis 3.kidneys ...only serositis is a bit controversial
The concept is a convoluted way of asking if you knew how VDJ recombination works, which is that it is actually an example of altering the DNA of the B/T lymphocyte.
Southern blot technique: So when they use a probe against some region, and outputting a size of 1.5 kb or 6 kb, this is telling you the size of the DNA fragment in each cell (doesn’t matter if they say J probe or constant region probe, they’re just saying they’re targeting some nucleotide sequence found in the Ig locus/TCR beta chain locus respectively for B/T cells).
I think the confusing part could be wondering how you know whether you’re partly through rearrangement (answer choices B thru D) or if it hasn’t occurred at all yet (correct answer). Here, the concept is that B cells undergo V(D)J rearrangement in the bone marrow, while T cells do it in the thymus, and it all happens at once. So a plasma cell in the blood like in Multiple Myeloma would have fully undergone recombination, while a T cell in the blood could either be fully educated (and have finished VDJ recombination) or immature (hasn’t started VDJ).
Since the T cell gene was 6 kb and definitely bigger than the 1.5 kb gene, the T cell hasn’t undergone recombination yet.
Weight loss - think cancer Hyponatremia - SIADH from small cell lung cancer Edema + JVD - SVC syndrome
So I think that issue of wrist extension and/or finger drop would be more radial nerve. However, there was more proximal weakness, so it would be C7.
"7-8 lay them straight", the pt couldn't "lay them straight" so it would be C7 root
According to FA 2019 Tricep Reflex is mediated by C6, yes C6 NOT C8, and C7 [In BOLD, implying it is more important].
This is a primary central nervous system lymphoma. Most commonly associated with HIV/AIDS; pathogenesis involves EBV infection.
Considered an AIDS-defining illness. Variable presentation: confusion, memory loss, seizures. Mass lesion(s) (may be ring-enhancing in immunocompromised patient) on MRI, needs to be distinguished from toxoplasmosis via CSF analysis or other lab tests. Toxo usually has multiple ring enhancing lesions.
{kind=link}
{kind=link}
Paraxial mesoderm means mesoderm surrounding the axis, aka the neural tube. They eventually form a pair of somites on either side. Somites then differentiate into:
Source
In this case, the patient is lacking spinous processes on top of having spina bifida. Maybe you were thinking spina bifida = neuropore defect, but what does this have to do with sclerotomes? This is what I found:
"Failure of closure of the caudal neuropore during embryogenesis will lead to spina bifida. This condition is always marked by a local lack of osteogenesis, or bone growth. The reason is that the correct differentiation and placement of underlying tissues (the spinal chord and spinal nerves and associated tissues) induce the osteogenesis, even small flaws in the underlying tissues can lead to a problem in the formation of the spine (vertebrae)." Source
So I'm guessing that when the question asks for "cause of the defect" they are talking about the vertebrae, not exactly the cause of spina bifida, which would be failure of neuropores to fuse. If that was an answer choice then def pick that, but the lack of vertebrae is due to lack of sclerotome fusion (because spina bifida could not induce it properly).