Welcome to aesalmon’s page.
Contributor score: 95
Comments ...
meningitis
I think its there.. I thought it was the lighter red/pink material (hyaline material)
And I thought the white streaks were the fibrosis like "streaked ovaries"in Turners.
+
samadmom
Apparently the histology looks like leydig cell hyperplasia but is actually called "pseudoademonatous clusters" and are reduced in number due to increased FSH and LH.
+
meningitis
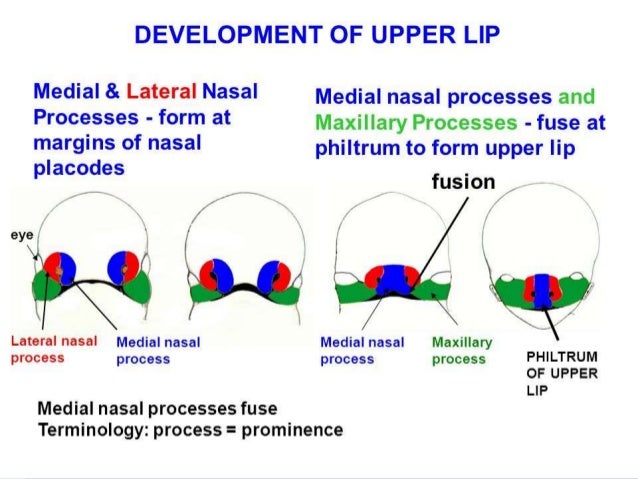
I think Cleft palate could also be due to failure of fusion of lateral and medial nasal prominences.. but since the baby had lip involvement and the lateral nasals can be seen, I went with failure of Maxillary and medial nasal fusion. Someone correct me if im wrong.
+4
snripper
@meningitis this is cleft lip, not cleft palate
+2
chaosawaits
@snripper, it's both. If you're palate looks like that, that's not normal fyi. The reason the answer is maxillary & median nasal prominences is because the question tells you to focus on the lip aspect of the patient's presentation.
+
drdoom
The prompt is only asking "what's the likely cause of obesity?" It's not that they're "allowing" him to eat more than exercise. (Few parents can monitor their kids that closely!) The prompt is only asking what's the most likely explanation for his 95th percentile weight and BMI (given that he otherwise appears normal); in the United States, the most likely explanation is eating way more than you expend.
+2
niboonsh
aka 'merica #firstworldproblems
+5
makinallkindzofgainz
If you are obese, it's because you have consumed calories in excess of your energy expenditure, end of story. (there are factors that affect your energy expenditure, but the simple statement is 100% true, unless you want to argue against the laws of thermodynamics). A is the only correct answer.
+1
castlblack
I think the reason they point out the average weight of the parents is because leptin disorders are inherited. It helps you eliminate that answer choice.
+2
jurrutia
Also, what is causing the splenomegaly? Cross out gastroduodenal A/V, gastric A/V, and pancreatoduodenal A/V since they have nothing to do with the spleen. All that's left is the splenic vessels, and you know it's a vein...
+1
psaucy
Thrombosis of the splenic vein causes the spleen to get congested with blood. You see splenomegaly + thrombosis = splenic vein errry time.
+1
jackie_chan
How are we supposed to know in the question the patients and providers are aware that they know what they are being given?
+1
haydenelise
I went back and forth about it, but in the end figured that they were aware since one regimen involved subQ injection + oral med and the other was subQ injection alone with no oral placebo.
+3
pippylongstock
This question is asking about the ‘S’ of FA Mnemonic for S. Pneumonia “MOPS”. Strep pneumo is the most common cause of sepsis in adults.
+3
emmy2k21
MOPS stands for meningitis, otitis, pneumonia, and SINUSITIS. It doesn't stand for sepsis. My guess as well is which is "more correct". It's about being able to identify encapsulated organisms and the spleen's role in immunity. Ha I chose E coli as well.
+7
et-tu-bromocriptine
emmy2k21 is correct, the S is for sinusitis. I was between E.coli & Strep Pneumo, but then recalled Sketchy putting the sickle on the 'encapsulated' knight in the Strep Pneumo video; Strep Pneumo is more associated with infecting sickle cell "functionally asplenic" patients.
+4
aneurysmclip
You could also recall that before splenectomy(ik this is a emergency splenectomy) we would want to give an encapsulated vaccine like the pneumococcal vaccine. this pushed me towards strep over ecoli
+2
yotsubato
It arises in the medulla and *passes* through the cortex because its invasive and malignant.
+13
benzjonez
I think that they just wanted you to notice the **calcifications**. Per FA, "calcifications are common in craniopharyngiomas," whereas I don't think you'd expect to see calcifications in a prolactinoma.
+21
epr94
also the option is prolactinoma not broad pituitary calcifications and he doesnt show any specific signs of high prolactin
+
madojo
It says hes coming in for constituional delay in growth and puberty, i took this to mean that he had low LH, FSH due to decreased GnRH from the prolactinoma. Why did they have to say low-normal serum gonadotropin, why not just say normal? fck u nbme
+2
madojo
It says hes coming in for constituional delay in growth and puberty, i took this to mean that he had low LH, FSH due to decreased GnRH from the prolactinoma. Why did they have to say low-normal serum gonadotropin, why not just say normal? fck u nbme
+1
ac3
@madojo I believe since suprasellar tumors can cause a mass effect on pituitary gland to decrease gonadotropin levels. Where as prolactinoma causes a rise in prolactin which downregulates gonadotropin secretion. Please correct me if I'm wrong
+2
macroorchidism
Yeah the low-normal threw me off...that and the fact the "kid" was 17. Thats basically an adult. I always thought the Craniopharynngiomas meant like children <10 y.o.
+
Subcomments ...
aesalmon
I totally skipped over the word "parentally" when taking this - ugh!
+22
imgdoc
Wow, I feel like such an idiot for getting such an easy question wrong...I skipped over parenteral and starting thinking about Cholera toxin MoA. ffs...
+
aesalmon
pg 338 of FA lists it under hypothyroidism but it does present as transient hyperthyroidism first
+9
hyperfukus
yep that was the key! Goiter is "HOT" but the remaining answer choices were still kind of bleh D was distracting the hell out of me i spent so long to convince myself to pick C and move on
+3
hello
Pasting nwinkelmann's comment as an addition: Choice "D" is wrong b/c "lymphomatous thyroid gland" = primary thyroid lymphoma (typically NHL, which is very rare) or Hashimoto's thyroid progression. Hashimoto's thyroiditis = lymphocytic infiltrate with germinal B cells and Hurthle cells, which upon continued stimulation, can lead to mutation/malignant transformation to B cell lymphoma. Both of these present with hypothyroidism with low T4 and high TSH (opposite of this patient).
+1
taediggity
I absolutely love your @liverdietrying, however the pathogenesis of postpartum thyroiditis is similar to Hashimoto's, so I think this person has postpartum thyroiditis and your explanation of transient thyrotoxicosis is spot on, which would also occur in postpartum thyroiditis
+16
pg32
I agree with @taediggity. Also note that women eventually recover from postpartum thyroiditis and typically become euthyroid again, which doesn't happen with Hashimoto's.
+
vulcania
In FA (2019 p. 338) it says that thyroid is usually normal size in postpartum thyroiditis, but the patient in this question had a thyroid "twice the normal size." I guess at the end of the day it doesn't matter which diagnosis is right for this question cause they both seem to lead to the same correct answer :)
+2
aesalmon
I actually thought that the posterior column findings were likely due to B12 deficiency - "subactue combined degeneration", due to malabsorption, as we see in this pt (. Turns out vitamin E can also cause symptoms which look like subacute combined degeneration: https://www.ncbi.nlm.nih.gov/pubmed/9012278, as does Copper (TIL): https://www.ncbi.nlm.nih.gov/pubmed/15249607
+3
jooceman739
Vitamin E deficiency causes posterior column findings and hemolytic anemia :)
+6
nwinkelmann
The way I think about it is that essentially, vitamin E is an anti-oxidant. Vitamin E deficiency = LOTS of oxidation, i.e. free radicals, which are toxic to most cells in the body (particularly myelination and RBCs). That's why it can be used with Alzheimer's patients.
+4
kevin
B12 would also affect lateral corticospinal tracts, vit E doesn't to my knowledge (b12 deficiency would also present with hyperreflexia but E deficiency just romberg sign, loss of proprioception and touch, ataxia)
+
aesalmon
I would also like to know if anyone can answer this question - I saw it as a Sattar "one day, one week, one month" kind of question. Its probably very simple but I still don't get it
+
bubbles
I posted a new comment explaining: basement membrane integrity is the strongest determinant of full fx recovery following pulmonary insult :)
+5
drdoom
You have to think about it this way: the basement membrane is the “scaffolding” on which [restorative] healing occurs. So, yes, stem cells (type II pneumocytes) would be involved in that healing process but they couldn’t restore the *normal* architecture (“no abnormalities”) without the ‘skeleton’ of the basement membrane telling them where to go, in what direction to grow, which way is “up”, etc. If the basement membrane is destroyed, you can still get healing, but it won’t be organized healing -- it’ll be *disorganized* healing, which does not appear as normal tissue. (Disorganized healing is better than no healing, but without a BM, the regenerating cells don’t have any “direction” and therefore can’t restore the normal architecture.)
+9
nwinkelmann
Yes, this a great summary to the post by @bubbles and the article he posted! Another way to think of the question is not, what causes repair, but what causes irreversible injury/fibrosis. That article explained an experiment that showed TGF-beta was necessary to initiate fibrosis, but if BM was intact and TGF-beta was removed, the fibrosis didn't persist, i.e. intact BM is protective against TGF-beta. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2645241/
+
seagull
ALK is increased in bone breakdown too. Prostate loves spreading to the lumbar Spine. It's like crack-cocaine for cancer.
+32
aesalmon
I think the "Worse at night" lends itself more towards mets, and the pt demographics lean towards prostate cancer, which loves to go to the lumbar spine via the Batson plexus. I picked Paget but i think they would have given something more telling if they wanted pagets, histology or another clue
+2
fcambridge
@seagull and aesalmon, I think you're a bit off here. Prostate mets would be osteoblastic, not osteolytic as is described in the vignette.
+17
sup
Yeah I chose Paget's too bcz I figured if it wasn't prostate cancer (which as @fcambridge said would present w/ osteoblastic lesions) they would give us another presenting sx of the metastatic cancer (lung, renal, skin) that might point us in that direction. I got distracted by the increased ALP too and fell for Paget :(
+1
kernicterusthefrog
@fcambridge, not exactly. Yes, prostate mets tends to be osteoblastic, but about 30% are found to be lytic, per this study: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2768452/ Additionally, the night bone pains point to mets, and Paget's is much more commonly found in the cranial bones and appendicular skeleton, than axial. This could also be RCC mets!
+
sweetmed
I mainly ruled out pagets because they said the physical examination was normal. He would def have other symptoms.
+4
cathartic_medstu
From what I remember from Pathoma:
Metastasis to bone is usually osteolytic with exception to prostate, which is osteoblastic.
Therefore, stem says NUMEROUS lytic lesions and sounds more like metastasis.
+5
medguru2295
If this is Metastatic cancer, it is likely MM. MM spreads to the spinal cord and causes Lytic lesions.
It is NOT prostate as stated above. While Adenocarcinoma does spread to the Prostate, it produces only BLASTIC lesions.
+
aesalmon
I agree, I picked H1 because such a common complaint for those on TCAs is Sedation, I figure it might be so commonly seen as to be the "most common" reason for noncompliance. I suppose the "hot as a hare...etc" effects would be more severe/annoying, but I didn't think they were more common.
+4
fcambridge
I just like to pretend that there's a reason this question is now in an NBME and no longer being used for the test. Hopefully they realized the idiocy of this question like we all do
+1
link981
Since it said cyclic, I thought of using, discontinuing, then using again. These people who write these questions need take some English writing courses so they can write with CLARITY. Cyclic is not the same as Tricyclic.
+6
waterloo
Incredibly awful question. one thought I did have when deciding between anticholinergic and antihistaminic - nortriptyline and desipramine are secondary amines that have less anti-cholinergic effects (from Sketchy Pharm) so maybe that's what they were getting at? That someone went out and made a new TCA drug that would have less anticholinergic effects.
+
victor_abdullatif
This isn't testing drug epidemiology; it's actually asking "which of these side effects are caused by TCAs and would be the worst to experience?"
+
tekkenman101
"worst to experience" is incredibly subjective lmao.
+1
aesalmon
Questions like this usually hinge on asking if you're going to follow the rules or not though, obviously the one asking her to lie and say she was her sister is wrong, but the correct answer is obviously breaking the hospice center's "policy" - presumably if the physician is sending her to hospice then they don't work there so why would the Dr. be able to just tell her its fine?
+6
hungrybox
Yeah, I got this one wrong with the same logic as you, aesalmon.
+1
emmy2k21
I genuinely interpreted this question as though the two women were in a relationship because of the quotes "my close friend". I figured significant others would be allowed to visit simply. Ha seems like I'm the only one who read too far in between the lines!
+9
dr_jan_itor
@emmy2k21 I also thought the quotes implied a lesbian relationship and that the patient was afraid to share this (they grew up at a time when it was heavily stigmatized). So i was thinking, of course you and your "special friend" can stay together. I know this is not just a phase
+10
et-tu-bromocriptine
Anything particularly wrong with A (Don't worry. I'll call you right away...")? It seemed like the most professional yet considerate answer choice.
Are we supposed to imply that they're partners based on those quotation marks around "close friend"? Because otherwise it seems like too casual and less professional than A, almost as if it's breaking policy.
+5
lilmonkey
I can swear that I saw this exact same question in UWORLD before. The only reason I got it right this time.
+1
docshrek
@lilmonkey can you please give the QID for the UWorld question?
+2
jakeperalta
Can someone explain to me why following hospital policy is the wrong answer? I'm so lost.And essentially how is this option any different from the last option where he asks her to say its her sister? Both go against hospital policy. Would greatly appreciate some insight yall.
+
jakeperalta
Can someone explain to me why following hospital policy is the wrong answer? I'm so lost.And essentially how is this option any different from the last option where he asks her to say its her sister? Both go against hospital policy. Would greatly appreciate some insight yall. P.s:it struck me as a romantic relationship as well, but it doesn't clear my doubt😓😭
+1
drschmoctor
@jakeperalta Following the hospital policy is wrong because it would be cruel and unnecessarily rigid to deny a dying woman the comfort of her closest companion. Also, It would be inappropriate to ask the Pt to lie.
What's the point of becoming a doctor if you have to follow some BS corporate policy instead of calling the shots and doing right by your patients?
+1
peridot
Ya kinda dumb that usually NBME usually tells us to never break the rules, yet here it's suddenly ok. But here the reason for this exception is that while only "family" is allowed, a lesbian relationship qualifies the "friend" as family (they just were never officially acknowledged as family/married due to stigma or state laws, which society recognizes today is dumb and outdated). It's a stupid technicality that her significant other isn't allowed to visit as a family member, so while we usually never want to break rules, this scenario follows the "spirit" of the rule. Plus it's a really extreme scenario where the woman is dying and just wants to spend her last moments with her loved one and it would be too cruel to deny someone that. There is no lie involved, which kinda leaves open the chance for the situation to be cleared up if worse comes to worst. This is different from E which is a straight up lie. Hope that helped.
+1
kavarthapuanusha
Well i am writing this after getting the answer wrong and after know the right answer , i kinda think its justified. Coz they mentioned its hospice, if in hospice any amount of pain medication is allowed , then this also should be allowed , afterall main aim is to comfort the patient! If it were may be elsewhere then following hospital policy may be right , but hospice always patients comfort first so makes sense!
Also its there in nbme 17 , so dont worry if you get it wrong .
+1
aesalmon
I agree, the article you linked states "signs of fetal hyperthyroidism such as tachycardia, intrauterine growth retardation, cardiac failure, and the development of fetal goitre"
I chose answer E during the exam - "Thyroid gland enlargement"
Still trying to understand how they linked cretinism to a case where the mother's hypothyroidism was well controlled, and then asked for the sequelae if her TSH increased. Maybe increased TSH is supposed to indicate worsening hypothyroid - low T3/T4 needing to be stimulated by TSH?
+
{kind=link}
Leydig cell hyperplasia, should also see fibrosis and hylinazation of the tubules but i'm not seeing it... ¯_(ツ)_/¯