Pulsatile mass in the abdomen combined with severe abdominal pain, decreased blood pressure, pail and lethargic all point to dissection of an abdominal aortic aneurysm. This would cause decreased femoral pulses due to loss of blood flow to the lower extremities.
Clostridium perfringins is a common cause of myonecrosis and would be described as a large gram(+) rod (FA2020p138).
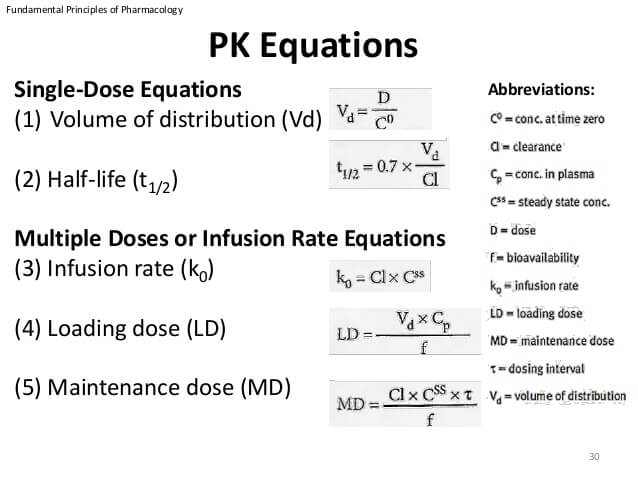
Here, we want to know loading dose which is equal to the volume of distribution x target concentration in plasma.
So our loading dose = 1.81L/kg x 10mg = 18.1mg/kg
She is a 55kg person so 18.1mg/kg x 55kg = 995.5 mg which approximates to 1000mg total loading dose.
Important Pharm Equations to Remember
Botulism toxin acts via proteases that cleave SNARE and prevent acetylcholine release at the neuromuscular junction (FA2020 p132). Thus, it does not directly affect the post-synatpric muscle cell. If you add external acetylcholine, you would still have a completely normal response. This eliminates all but two answers.
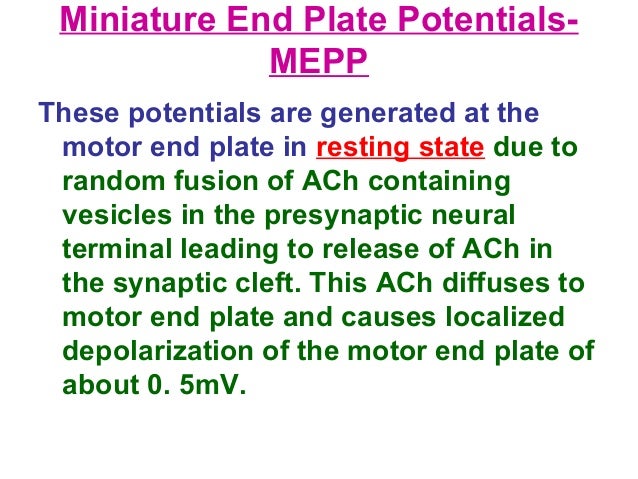
The end plate potential (EPP) would be affected by botulism toxin because the end plate potential is the change in voltage that occurs at the postsynaptic muscle motor endplate after an action potential in the motor neuron axon triggers release of many acetylcholine vesicles. Normally, an action potential in the motor neuron will cause influx of calcium that leads to fusion of Ach vesicles (requiring SNARE) and exocytosis, releasing large quantities of Ach into the synapse which can then bind and trigger an EPP in the muscle. With botulism, fusion of the Ach vesicles is inhibited so less Ach is released and the EPP is blunted. Notably, the voltage is the same as the mEPP which is the voltage after random occurrence of Ach release (see below).
A miniature end plate potential (mEPP) is the voltage change that occurs when one vesicle of acetylcholine is released. These occur randomly. mEPP would not be affected by botulism toxin because it is the produce of random fusion of a vesicle which could still occur after administration of botulism toxin.
Here is an image reminding the difference between EPP and mEPP.
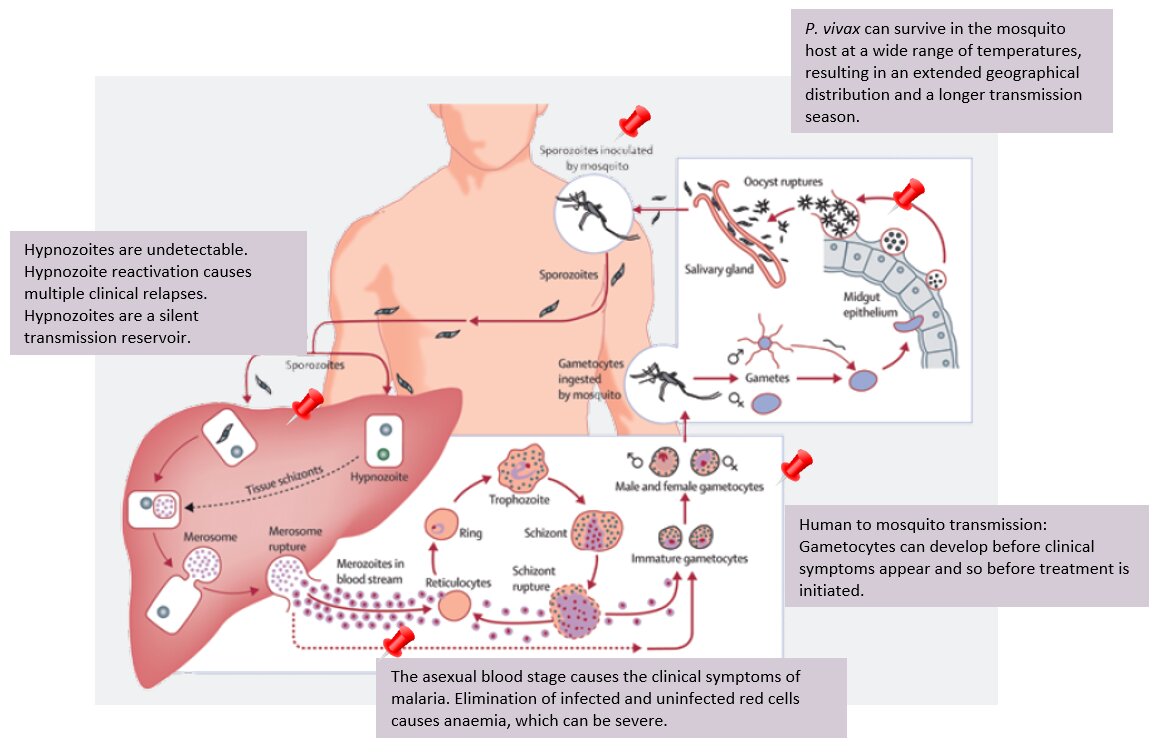
Chloroquine does not adequately kill the dormant liver form of malaria (hypnozoite), and thus for infections that have a hypnozoite stage treatment requires addition of primaquine (which does adequately kill hypnozoites) to prevent relapse from release of the infection back into the blood. [FA2020 p157]
Hypnozoites are the dormant form of malaria in the liver (think hypno as in sleeping from hypnosis). Plasmodium vivax and ovale have the hypnozoite stage and thus require the addition of primaquine.
Clostridium tetani and Cornybacterium diphtheriae are part of an inactivated toxoid vaccine with Bordatella pertussis (Tdap and DTap consist of Tetanus toxoid, diptheria toxoid, and acellular pertussis, hence ap)
FA2020 p111
Lesion of the hippocampus results in anterograde amnesia (FA2020 p511, think 50 First Dates kind of forgetting).
Also, the hippocampus is one of the most vulnerable places to ischemic injury (pyramidal cells of the hippocampus, p512)
FA2020 p144
An USMLE testable fact about salmonella species is that antibiotic use actually prolongs the excretion of the organism. Fun fact(?) for memorization as there is no clear answer as to why that I could find.
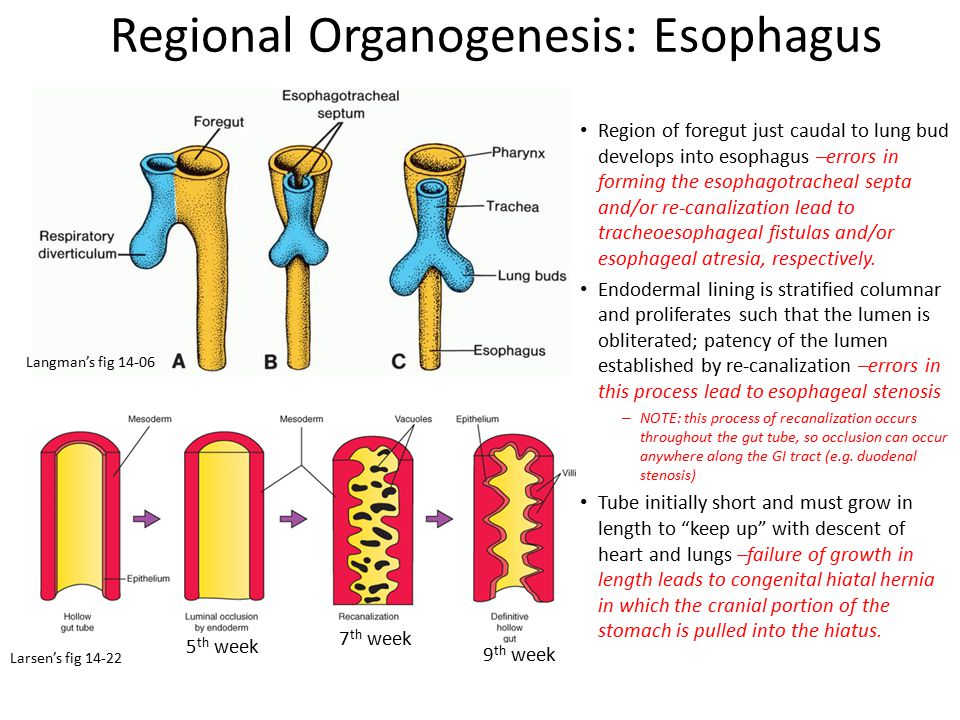
The esophagus is a component of the foregut of the gut tube, which is lined with endoderm. Pure esophageal atresia can occur due to failure to recanalize. (FA2020 p359) See here for slide explanation.
The girl is having absence seizures (staring into space, 3 second bursts of 3/sec spike-and-wave activity). The first-line treatment for absence seizures is ethosuximide. (FA2020 p544 and 517)
He presents with an anticholinergic toxidrome: hot as a hare, dry as a bone, mad as a hatter (FA2020 p241, the anticholinergic toxidrome is the same as an atropine overdose and jimsonweed actually contains atropine).
The antidote for antichlinergics is phyostigmine, an acetylcholinesterase inhibitor that acts as an indirect cholinergic agonist. (FA2020 p240)
Cimetidine is one of the cytochrome p450 inhibitors which would allow increase of the concentration of diazepam to toxic levels by inhibiting its elimination. (https://en.wikipedia.org/wiki/Diazepam)
SICKFACES.COM when I Am Really drinking Grapefruit Juice (FA2020 p252)
Ondansetron is a powerful antiemetic that works by antagonizing serotonin 5HT3 receptors. It is given for postoperative nausea and chemotherapy-induced nausea (FA2020 p400)
Give mesna with cyclophosphamide to prevent hemorrhagic cystitis (FA2020 p251)
This is metastatic renal cell carcinoma (FA2020 p605) for the following reasons:
Yellow nodules (cholesterol deposits) on the achilles tendons have a very high association with Type II familial dyslipidemia, or familial hypercholesterolemia. This is caused most often by a defect in the LDL receptor function. (FA2020 p94)
DISTRIBUTIVE SHOCK (I.E. SEPTIC OR ANAPHYLAXIS) ARE THE ONLY SHOCKS WITH INCREASED CARDIAC OUTPUT!
FA2020 p310
This man presents with hypothermia (septic shock can present with hyper or hypothermia), tachycardia, and low blood pressure with increased cardiac output, characteristic of septic shock. Further distributive shock is associated with severe decrease in systemic vascular resistance while other forms of shock have increased systemic vascular resistance.
I don't like how they are asking this, but I think what they are getting at is that after the stent placement ("subsequent to the stent placement") there will be reperfusion injury to the myocardial tissue which occurs through free radical injury and therefore membrane lipid peroxidation is the best answer (FA2020 p210 mentions membrane lipid peroxidation as a mechansism of free radical damage and lists reperfusion injury after thrombolytic therapy as a type). Elevations in the cardiac enzymes I assume are because of the injury to the cells.
The key here is "wound healing". TGF-beta is a vital cytokine in the healing process as well as in attenuation of immune response (FA2020 p216)
FGF, TGF-beta, VEGF, PDGF, EGF (all GROWTH factors ending in GF which promote healing) as well as metalloproteinases (for remodeling) are vital in the wound healing process.
TGF-beta and IL-10 are the two "resolution" cytokines vital in attenuating the immune response. FA2020 p108 has important cytokines.
In androgen insensitivity syndrome, the testes may descend and push through into the labia majora. Thus the labia majora corresponds to the scrotum. (FA2020 p639)
Here is a diagram of corresponding embryological structures. FA2020 p622 discusses sexual differentiation but doesn't go as in depth with which exact structures correspond.
The basics of this question are what are the major chemotactic factors that attract neutrophils to the site of injury.
These are: IL-8, C5a, LTB4, kallikrein, and platelet activating factor
FA2020 p406 and 215
Important cytokines are on p108
The Congo Red staining showing characteristic birefringence (usually described as apple green) is indicative of amyloid (FA2020 p212). Her findings are characteristic of secondary amyloidosis with serum amyloid A which can cause restrictive cardiomyopathy and nephrotic syndrome and is associated with rheumatoid arthritis.
Amyloid protein composition is misfolded aggregates of beta-pleated sheets.
These individuals have a poluymorphism in the breakdown pathway of 6-MP. Like most polymorphisms in drug breakdown pathways, this will lead to buildup of toxic metabolites unless the drug dose is decreased (i.e. the 6-MP will be shunted into the pathway that makes the toxic 6-thioguanine).
6-MP and its prodrug azothioprine inhibit purine synthesis (FA2020 p36 and p440).
Alendronate is a bisphosphonate which acts as a pyrophosphate analog and binds hydroxyapatite in bones and inhibits osteoclast activity. (FA2020 p486)
As a general rule, most drugs of osteoporosis inhibit osteoclast activity and bone resorption somehow (the bisphosphonates, calcitonin mimetics [directly bind a receptor on osteoclasts], estrogens/SERMs [inhibit PTH mediated bone resorption and cytokine secretion], Denosumab [mAb which inhibits RANKL which typically activates osteoclasts]). The ONLY FDA approved medication which has the ability to stimulate bone formation is teriparatide.
(FA2020 p462 osteoporosis)
This is a Congenital Diaphragmatic Hernia (FA2020p370).
Conginital diaphragmatic hernias are caused by a congenital defect of the pleuroperitoneal membrane which allows contents of the abdominal cavity to herniate upward, and displace the contents of the thorax (hence why our baby has displacement of the mediastinal contents to the right). This also leads to lung malformation and respiratory distress (hence the low apgar scores). Because the stomach is likely herniates upward, a nasogastric tube placed would appear in the left mediastinum (because that is where the stomach is). Further, there is an absence of bowel gas in the abdomen likely because the bowels are herniated into the thorax.
Water does not require transport proteins or energy for absorption, and transepithelial transport means it must go through the epithelial cells. C is the best match.
This is neonatal physiologic jaundice (FA2020 p393), which is primarily due to immature UDP-gluconuryosyltransferase causing an unconjugated bilirubinemia. The mechanism is decreased conjugation of bilirubin.
This is G6PD deficiency. (FA2020 p422)
G6PD deficiency causes a hemolytic anemia when individuals are exposed to antimalarials due to the increased oxidative stress. This is due to the deficiency in replenishing NADPH which is necessary to replinish reduced glutathione which aids in quenching free radicals.
Propanolol is a nonselective beta blocker:
Here's how I thought through this. problem with DCML (absent proprioception and vibration sense), problem with deep tendon reflexes (DRGs), ataxic gait (spinocerebellar pathway), mild weakness (motor neurons). The only thing that all of these pathways have in common is that they all use myelinated afferents.
I don't know if Guillan Barre would actually present like this, but you don't have to know what the illness is to figure the question out.
Why no sweating? I mean I get Ecstasy is probably the drug of choice before an all night dance party (lol) but don't understand why there would be cold extremities and no sweating when is FA it says hyperthermia and rhabdo????
DOSE x F = AUC x CL
(F= Bioavailability)
If dose is constant and F is increased for Drug X then AUC would increase.
Lol i thought trauma would hit more superficial structure than deep.. haha
Why wouldn't the body down-regulate the conversion of FT4 into FT3? Is that conversion just constitutively activated? Since FT3 is more potent than T4, it would make sense for the body to turn that conversion down...that was my reasoning...obviously not correct, but idk why that wouldn't be the case. Anyone have insight?
Why wouldn't the body down-regulate the conversion of FT4 into FT3? Is that conversion just constitutively activated? Since FT3 is more potent than T4, it would make sense for the body to turn that conversion down...that was my reasoning...obviously not correct, but idk why that wouldn't be the case. Anyone have insight?
Does anyone have a good explanation for why decreased levels of inhibin is wrong? From my understanding, inhibin and activin work together, in that inhibin binds and blocks activin leading to decreased feedback on hypothalamus and activin increases FSH and GnRH production.. thus, if you decrease inhibin then you would have increased activin which would lead to increased GnRH and FSH, right? I found one article talking about it in regards to puberty, but it seems to be a hypothesis/not confirmed at this point... is that why? But still... how do I rule it out on a test?
I was trying to figure out how are the catecholamines cause the K shift into the cells. I was not seeing the connection at first. normally in old NBMEs and Uworld questions- Insulin is causing K+ to enter the cells. then I remember seeing the sketchy band camp and in the far right of the sketch there is B2 activation = beta 2 tuba or something.. anyway beta 2 is found on pancreatic beta cells, catacholamines activate beta 2 on pancreatic beta cells which will cause insulin to be released. insulin released causes K to be driven inside the cells, causing the hypokalemia
references:
-FA 2019 pg 238 Beta 2 --> increase in insulin release and increase cellular K+ uptake.
-Linda S. Costanzo's physiology text:image showing insulin and beta agonist driving K+ into the cells
And just incase you were as curious as I am and wanted to know what tautomerism is.... A tautomer is an isomer , and isomers are compounds that have the same number of atoms of the same element but different structural arrangemennts
A NOTE TO SELF : DO NOT PICK THIS ANSWER IN THE EXAM
And just incase you were as curious as I am and wanted to know what tautomerism is.... A tautomer is an isomer , and isomers are compounds that have the same number of atoms of the same element but different structural arrangemennts
A NOTE TO SELF : DO NOT PICK THIS ANSWER IN THE EXAM
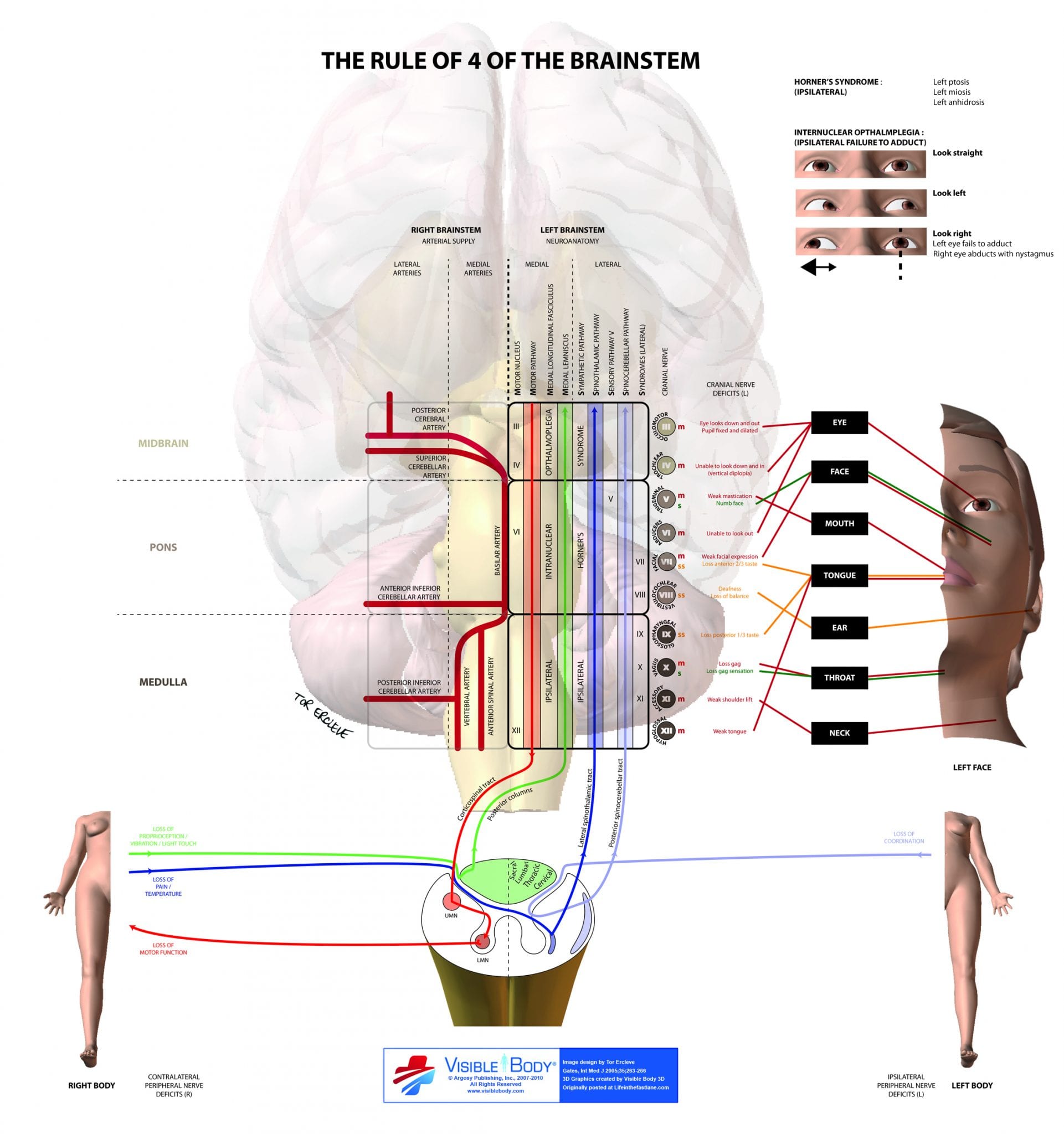
"Simple rules of the brainstem" (credit to our anatomy gods at UofL for organizing, also this image is fucking great for visual learners):
As both may occur after trauma Just recall : *Synovial Cyst (ganglion cyst ) - forms a fluctuant mass
*Myositis ossificans - as in the question - forms a " very firm " mass
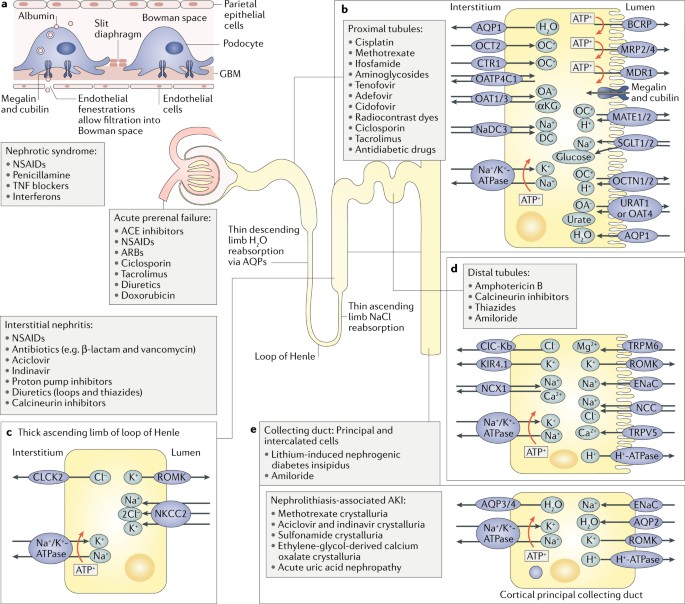
Aminoglycosides are nephrotoxic; nephrotoxic chemicals/drugs cause acute tubular necrosis (ATN), characterized by damage to the PCT. ATN causes the formation of brown, muddy, granular casts in the urine. The fact that this patient is a quadriplegic might be suggesting that they have a lower volume of distribution for the drug (and therefore higher blood concentrations).
All of the features described of this patient would be expected of a 68-year-old man. Shorter, less intense orgasms, as well as increased time needed between sex could be related to a slight drop in testosterone with age. However, he continues to grow hair well (feet and toes), implying that he hasn't dramatically lost testosterone production. His prostate is slightly enlarged, which could imply benign prostatic hyperplasia, but this should not directly impact his sexual function.
Somatostatin is normally secreted by D cells in the pancreatic islets and GI mucosa. It basically blocks everything GI-related ("encourages somato-stasis"): decreased gastric acid & pepsinogen secretion, decreased pancreatic and small intestine fluid secretion, decreased gallbladder contraction, decreased insulin & glucagon release.
Decreasing gastrin release blocks the increase of GI motility (increased GI motility is the inherent problem of diarrhea).
The drug in the question is probably octreotide.
This is acute hemolytic transfusion reaction, a type II hypersensitivity where pre-formed IgM antibodies bind to incompatible ABO antigens on donor RBCs, which causes intravascular hemolysis. Rh incompatibility, like colonelred_ said, comes more into play with Rh-compatibility of pregnancy and it is due to IgG antibodies, which more often cause extravascular hemolysis since splenic macrophages have those Fc-gamma-R receptors to bind whatever IgG has caught. Extravascular doesn't cause that hypotension, fever, flank pain associated with hemoglobinuria since the macrophages hold on to the degraded RBCs and convert it to biliverdin, which can safely be excreted by the liver.
Why not a tear in the sciatic nerve? especially since it radiates down to the leg
Acute MI and mitral regurg (from the murmur) leads to LV failure and backflow of blood into the lungs.
This leads to increased pulmonary hydrostatic capillary pressure. This will lead to excess volume leaking from the pulmonary capillaries into the interstitial and this will manifest as pulmonary edema (crackles).
Pulmonary edema will interfere with gas exchange leading to hypoxemia.
Acute MI and mitral regurg (from the murmur) leads to LV failure and backflow of blood into the lungs.
This leads to increased pulmonary hydrostatic capillary pressure. This will lead to excess volume leaking from the pulmonary capillaries into the interstitial and this will manifest as pulmonary edema (crackles).
Pulmonary edema will interfere with gas exchange leading to hypoxemia.
This question sounded like botulism, anybody knows why is tetanus?
This question sounded like botulism, anybody knows why is tetanus?
Note: IL-12 receptor deficiency, or a defect in the Interferon Gamma receptor
Think Disseminated Mycobacterial and Fungal Infections . Also salmonella *
First step is to make the presumptive diagnosis of osteoporosis from the clinical vignette . ( The supposed subtype in our patient is postmenopausal osteoporosis)
After this the next step is to make an association with the lab findings The primary defect is a deficiency of estrogen . Normally estrogen decreases osteoclast activity by
Net effect of losing estrogen is increased osteoclast activity ,and in this question by extension RANK L concentration .
NOTE : ALP which is an indicator of osteoblast activity does not change/ increase in osteoporosis , as such avoid all options with an increase in osteoblast activity
A: Gonadal mosaicism | Present in child, not parent → would not have family history of disease
B: Incomplete penetrance | Correct! Half of children affectd, skips a generation → AD inheritance likely.
C: Nonpaternity → Prader-Willi
D: Somatic mosaicism | Present in parent, not child → would not have family history of disease
E: Variable expressivity | Affected patients have varying disease severity → Rule out b/c mother is unaffected
Due to "contraction alkalosis" loop diuretics cause volume contraction, thats why you give them.
As a result, there is increase angiotensin II release, increase in Na+/H+ exchange in the PCT (a function of increase angiotensin II), and then increased HCO3- reabsorption, leading to alkalosis
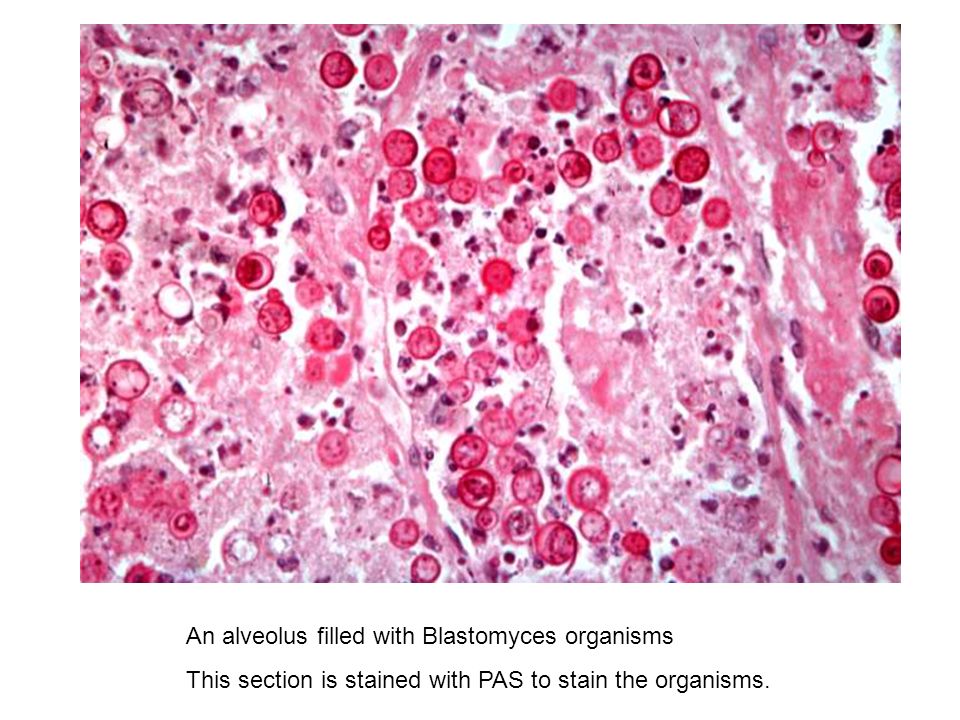
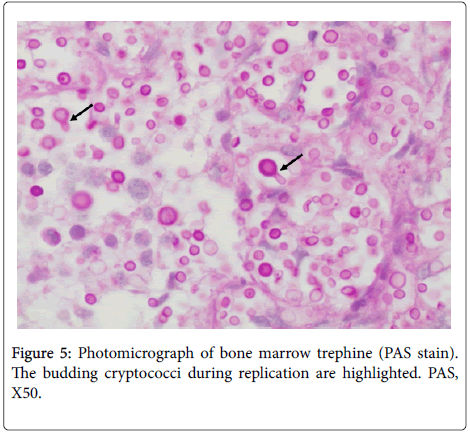
Can someone please explain what we're seeing on the histo slide? I chose the correct answer because I was thinking fungus because of the immunocompromise and neutropenia (and I thought PAS was used for aspergillus), but I don't see anything fungus-related on that slide.
The two sections of the nephron most susceptible to hypoxic conditions are the 1) proximal convoluted tubule and the 2) mTAL (medullary section of the thick ascending loop of Henle)
This ratio is used to determine appropriate production of lung surfactant, so this baby would not have appropriate production of surfactant if birthed at the time of the ratio calculation. It would go into neonatal respiratory distress syndrome.
TL;DR: surfactant decreases lung recoil, so the lack of surfactant in this baby will cause an increased recoil which will decrease the functional residual capacity (FA 2020 p661-662)
Surfactant is necessary to decrease surface tension of alveoli and increase compliance of the lungs (remember when the lungs have greater compliance, this makes the lungs easier to fill). Surfactant also helps to prevent alveolar collapse as the lack of surfactant allows there to be varying surface tensions between large and small alveoli (Law of Laplace), so lack of surfactant would lead to widespread atelectasis (alveolar collapse). Because surfactant serves to decrease these forces which normally favor collapse of the lung, it also serves to decrease the lung recoil.
Lack of surfactant in a baby = increased alveolar surface tension, lower compliance, more alveolar collapse, more recoil (less residual volumes)
Total lung capacity is unchanged because with enough force you can still expand the lungs to full capacity.
This patient with a history chronic hypertension is most likely suffering from left heart failure (decreased cardiac outpout), causing the blood to back up in the lungs (Crackles are heard bilaterally, shortness of breath) and that resulting into increased afterload for the right side of the heart, raising the pressure in the right heart chambers, which get transmitted back to central vein.
This patient with a history chronic hypertension is most likely suffering from left heart failure (decreased cardiac outpout), causing the blood to back up in the lungs (Crackles are heard bilaterally, shortness of breath) and that resulting into increased afterload for the right side of the heart, raising the pressure in the right heart chambers, which get transmitted back to central vein.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tetracyclines are bacteriostatic and bind the 30S subunit to prevent attachment of aminoacyl-tRNA. Doxycycline and other tetracyclines are commonly used for refractory acne.
Other answers: