why could the answer not be G6PD (also unconjugated) Or abnormal synthesis (what does this one even refer to?)
is this question asking what we physically pass through or by?
I thought ablation of the av node was a tx for a fib not heart block?
according to uworld hypersensitivity pneumonitis is due to dust and that was also an option....
how do we know parakeets cause hypersensitivy pneumonitis
His tidal volume was 500 mL. End-expiratory was +5 cm and end-inspiratory was +25. We were supposed to use the difference in airway pressure, and not the end-inspiratory pleural pressure (+20).
Compliance = ΔV/ΔP = 500 / 20 = 25 mL/cm H2O
Basement membrane integrity is the determinant of full lung recovery following pulmonary insult.
Summary:
(1) loss of basement membrane integrity is critical in determining the “point of no return,” and contributes to the inability to reestablish normal lung architecture with promotion of fibrosis;
(2) loss of epithelial cells, endothelial cells, and basement membrane integrity in usual interstitial pneumonia associated with idiopathic pulmonary fibrosis leads to destroyed lung architecture and perpetual fibrosis;
(3) transforming growth factor-β is necessary, but not entirely sufficient, to promote permanent fibrosis;
(4) persistent injury/antigen/irritant is critical for the propagation of fibrosis;
(5) idiopathic pulmonary fibrosis is an example of a process related to the persistence of an “antigen(s),” chronic inflammation, and fibrosis; and
(6) unique cells are critical cellular players in the regulation of fibrosis.
citation: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2645241/
Basement membrane integrity is the determinant of full lung recovery following pulmonary insult.
Summary:
(1) loss of basement membrane integrity is critical in determining the “point of no return,” and contributes to the inability to reestablish normal lung architecture with promotion of fibrosis;
(2) loss of epithelial cells, endothelial cells, and basement membrane integrity in usual interstitial pneumonia associated with idiopathic pulmonary fibrosis leads to destroyed lung architecture and perpetual fibrosis;
(3) transforming growth factor-β is necessary, but not entirely sufficient, to promote permanent fibrosis;
(4) persistent injury/antigen/irritant is critical for the propagation of fibrosis;
(5) idiopathic pulmonary fibrosis is an example of a process related to the persistence of an “antigen(s),” chronic inflammation, and fibrosis; and
(6) unique cells are critical cellular players in the regulation of fibrosis.
citation: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2645241/
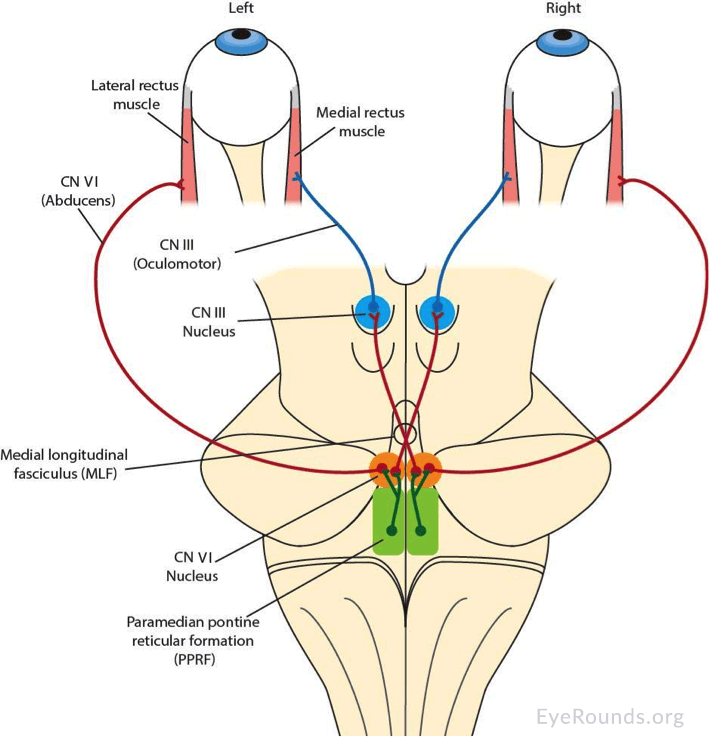
Here’s another very nice one that superimposes the pathway onto a simplified brainstem drawing (nice for the anatomical relations):
https://webeye.ophth.uiowa.edu/eyeforum/cases-i/case252/Fig2-INO-LRG.png
Source article:
https://webeye.ophth.uiowa.edu/eyeforum/cases/252-internuclear-ophthalmoplegia.htm
To see even more, try google image search on “medial longitudinal fasciculus”:
https://www.google.com/search?q=medial+longitudinal+fasciculus&tbm=isch
1) Superficial (first-degree) = Epidermis ~ presents as red skin without blisters
2) Superficial partial thickness (second-degree) = Extends into superficial (papillary) dermis ~ Presents with redness with clear blister & blanches with pressure
3) Deep partial thickness (second-degree) = Extends into deep (reticular) dermis ~ presents as yellow or white skin with less blanching. May be blistering.
4) Full thickness (third-degree) = Extends through entire dermis ~ presents as stiff and white/brown skin. No blanching.
5) Fourth-degree = Extends through entire skin, and into underlying fat, muscle and bone ~ presents as black skin; charred with eschar
1) Superficial (first-degree) = Epidermis ~ presents as red skin without blisters
2) Superficial partial thickness (second-degree) = Extends into superficial (papillary) dermis ~ Presents with redness with clear blister & blanches with pressure
3) Deep partial thickness (second-degree) = Extends into deep (reticular) dermis ~ presents as yellow or white skin with less blanching. May be blistering.
4) Full thickness (third-degree) = Extends through entire dermis ~ presents as stiff and white/brown skin. No blanching.
5) Fourth-degree = Extends through entire skin, and into underlying fat, muscle and bone ~ presents as black skin; charred with eschar
Tanner stages start at TEN years old
Stage I:
Stage II (2): stage II starts at 11 y/o (II look like 11)
Stage III (3): starts at 13 y/o
Stage IV (4): starts at 14 y/o
Stage V (5): 15 y/o
Tanner stages start at TEN years old
Stage I:
Stage II (2): stage II starts at 11 y/o (II look like 11)
Stage III (3): starts at 13 y/o
Stage IV (4): starts at 14 y/o
Stage V (5): 15 y/o
This more likely to be diuretics rather than laxatives b/c
the lab study shows a renal dysfunction (BUN & Creatinine are elevated)
Most likely the patient abused loop diuretics; also knows to cause contraction alkaloids, along with renal problems such as interstitial nephritis
Premie has no surfactant
Angiotensin II - generated in hypovolemia
Dipalmitoyl lecithin aka dipalmitoylphosphatidylcholine lung surfactant
Phosphatidylinositol 4,5-bisphosphate aka PIP2 Gq receptor pathway
Phosphatidylserine -involved in intrinsic apoptosis when exposed on extracellular surfaces
Sphinogmyelin - composes myelin and also has roles in signal transduction, apoptosis. Lecithin: Sphingomyelin ratio >2 indicates mature fetal lungs.
The damage is in the L midbrain in the area affecting the corticospinal tract. Because it is in the midbrain, decussation in the pyramids (medulla) so it will show ipsilateral dysfunctional motor signs.
Photo of midbrain and important areas: shorturl.at/myHLR
Swelling of the cell (e.g., hydropic degeneration): tissue ischemia → decreased ATP production → decreased Na+/K+ ATPase and Ca2+pump activity → diffusion of Na+ and water into the cell → cellular swelling
Swelling of the cell (e.g., hydropic degeneration): tissue ischemia → decreased ATP production → decreased Na+/K+ ATPase and Ca2+pump activity → diffusion of Na+ and water into the cell → cellular swelling
{kind=link}
{kind=link}
why not myastehnia for this one? They put some LE weakness in the stem as well so that before respiratory depression made me skeptical of it being a pure descending paralysis and I went with MG instead .