1) Alcohol withdrawal --> seizure
2) Seizure --> increased release of catecholamines (https://www.ncbi.nlm.nih.gov/pubmed/6538024), also BP of 180/100 indicates high levels of catecholamines
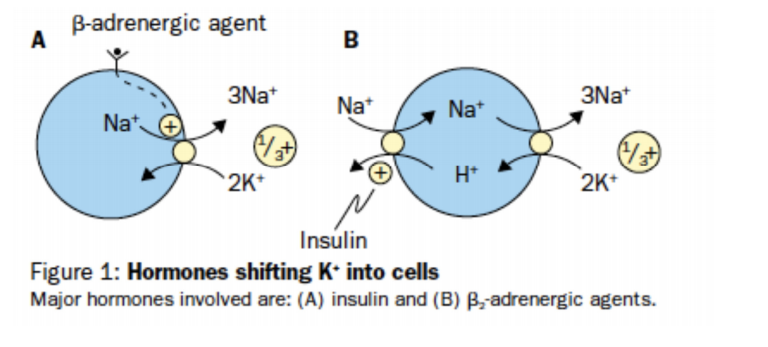
3) Major hormones that shift K+ intracellularly are insulin & beta-2-adrenergic agonists (e.g. epinephrine (http://www.clinicalguidelines.scot.nhs.uk/media/1286/fig1picu007.png)
4) Also they are asking why serum K+ is low, NOT why urine K+ is high
Emedicine says: Delirium tremens (DTs) is the most severe form of ethanol withdrawal, manifested by altered mental status (global confusion) and sympathetic overdrive (autonomic hyperactivity), which can progress to cardiovascular collapse.
Also ref. https://pubs.niaaa.nih.gov/publications/aa05.htm
I assume the patient has Delerium tremens, had a seizure, and now is hypertensive because of the "sypathetic overdrive", with excess secretion of catecholamines, thus the hypokalemia.
Can someone explain why does this patient have hypokalemia?
in the other hand , urine potassium is high enough , so if seizures =>rhabdomyolysis => myoglobinuria => ATN => high potassium excretion , why not?
This maybe to late for anyone but here was my train of thought Catecholamine : 1. increases insulin release --> glu and K will enter cells. Causing hypokalemia in the plasma 2. Can trigger the beta 1 receptor causing the release of Renin---> Angiotensin 2 (can be contributing / causing an increase in BP)--> aldosterone --> you waste K in the urine.
• This patient with alcohol withdrawal most likely developed acute hypokalemia due to stress-related beta-adrenergic hyperactivity, which causes potassium to shift intracellularly. • Severe physiologic stress (eg, myocardial infarction, head injury) results in significant endogenous catecholamine (eg, norepinephrine, epinephrine) release. Epinephrine activates the beta-2 receptor, leading to increased activity of the sodium-potassium ATPase pump and the sodium-potassium-2-chloride cotransporter, both of which transport potassium intracellularly. Adrenergic activity also stimulates the release of insulin, which further promotes intracellular potassium shifting.
Source: UWORLD
Alcohol withdrawal - - > increased catecholamines - - > increased insulin (via B2) - - > cellular uptake of K+ - - > hypokalemia
{kind=link}
submitted by poormedstudent(14)
I was trying to figure out how are the catecholamines cause the K shift into the cells. I was not seeing the connection at first. normally in old NBMEs and Uworld questions- Insulin is causing K+ to enter the cells. then I remember seeing the sketchy band camp and in the far right of the sketch there is B2 activation = beta 2 tuba or something.. anyway beta 2 is found on pancreatic beta cells, catacholamines activate beta 2 on pancreatic beta cells which will cause insulin to be released. insulin released causes K to be driven inside the cells, causing the hypokalemia
references:
-FA 2019 pg 238 Beta 2 --> increase in insulin release and increase cellular K+ uptake.
-Linda S. Costanzo's physiology text:image showing insulin and beta agonist driving K+ into the cells